


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-

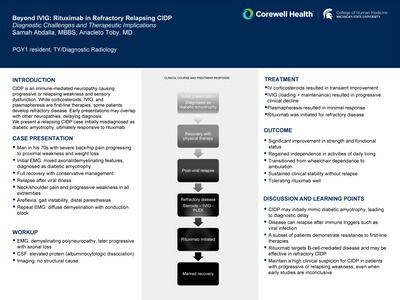
Not Just Bad Luck: Pneumococcal Meningitis in a Vaccinated Adolescent Leading to the Diagnosis of a CSF Leak
Krupa Patel, Hannah Campbell, and Michael Metz
Publication Date: 5-8-2026
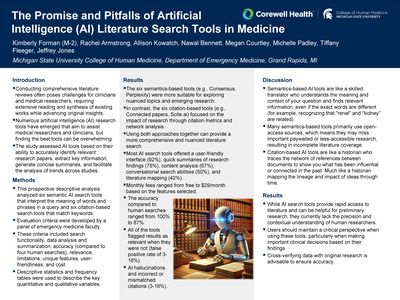
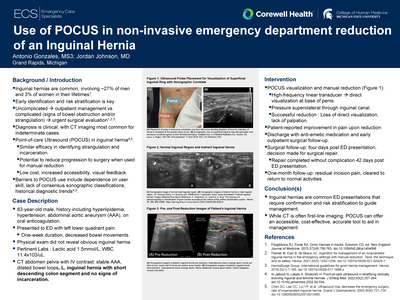
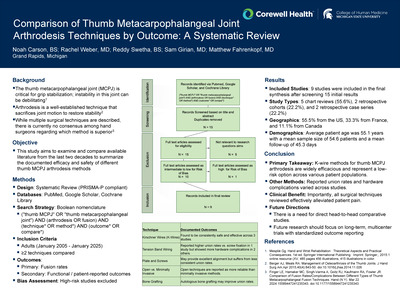
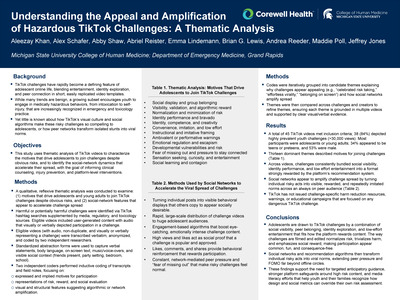
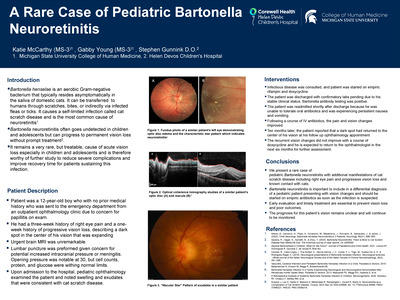
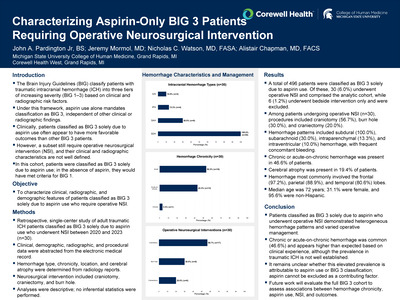
Pneumococcal meningitis is the most common cause of bacterial meningitis in children, with the highest incidence in those under five years of age. Although pneumococcal conjugate vaccines have reduced invasive disease, infections continue to occur among fully vaccinated individuals. Streptococcus pneumoniae is an encapsulated gram-positive coccus that evades host immunity and can cause severe central nervous system infection following bloodstream invasion and traversal of the blood-brain barrier. Risk assessment often emphasizes vaccination status and immunodeficiency, with less attention given to structural predisposing factors. Cerebrospinal fluid leaks are an underrecognized cause of breakthrough pneumococcal meningitis and may be clinically occult, increasing the risk of recurrence. We report a case of pneumococcal meningitis in a fully vaccinated adolescent with an occult CSF leak.
An otherwise healthy, fully vaccinated 14-year-old male presented to an outside hospital with one day of headache, confusion, altered mental status, recurrent vomiting, and fever. He was transferred to Pediatric ICU at Helen DeVos Children's Hospital for further management of suspected meningitis. A lumbar puncture showed low glucose, elevated protein and significant pleocytosis consistent with bacterial meningitis. A peripheral blood culture and PCR meningitis/encephalitis panel was positive for Streptococcus pneumoniae. CT Brain showing cerebral edema and meningitic inflammation. An immunodeficiency evaluation was unremarkable.
Pneumococcal meningitis may occur in fully vaccinated, previously healthy adolescents in the presence of predisposing anatomical abnormalities. Cerebrospinal fluid leaks are an important and frequently underrecognized risk factor for invasive pneumococcal disease, even in the absence of facial trauma or immunocompromising conditions. Breakthrough bacterial meningitis should prompt evaluation for structural defects, including CSF leak. Early diagnosis and definitive management may reduce the risk of recurrent invasive infection.
-

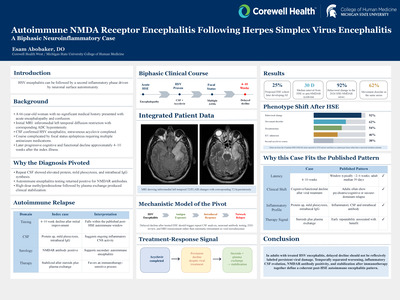
Ceftriaxone-Induced Immune Hemolytic Anemia and Subsequent Disseminated Intravascular Coagulation: A Case Report
Hunter T. Pham, Jennifer Bach, Christian Kolacki, Jeffrey Jones, and Nathan DeBruine
Publication Date: 5-8-2026
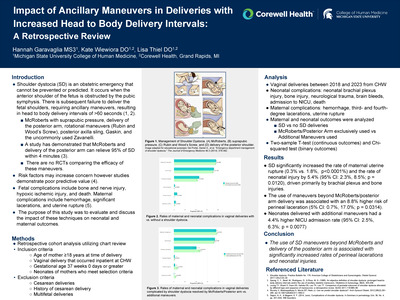
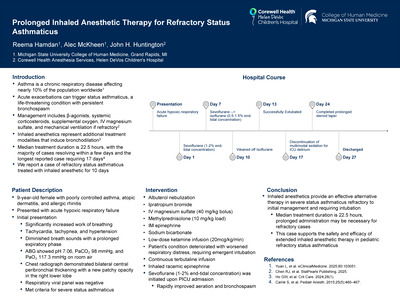
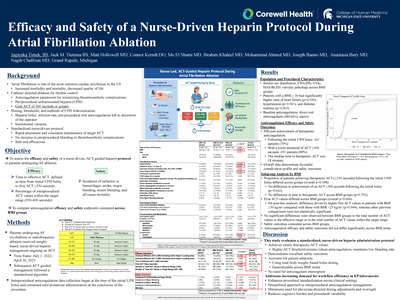
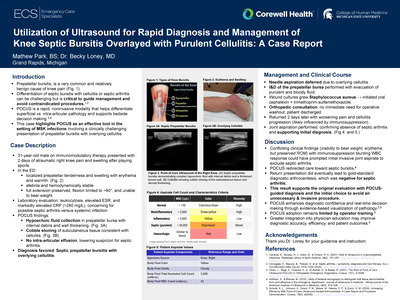
Drug-induced immune hemolytic anemia (DIIHA) is a rare but severe reaction in which drug-dependent antibodies rapidly destroy red blood cells, causing illness that can progress to fulminant, life-threatening shock. Ceftriaxone is among the antibiotics most frequently implicated and has been associated with abrupt deterioration and death despite its widespread use as a broad-spectrum agent. This report describes ceftriaxone-induced DIIHA complicated by disseminated intravascular coagulation (DIC) in an older adult, highlighting the catastrophic potential of this reaction in the emergency setting.
A 78-year-old woman with type 2 diabetes mellitus presented to a rural emergency department with acute drowsiness, vomiting, abdominal pain, and transient neurologic deficits, prompting a stroke code. Initial imaging, including CT head, CT angiography, and CT perfusion, was unremarkable, while CT chest showed mild interstitial changes concerning for pneumonia, and she was started on ceftriaxone and azithromycin. Within 30 minutes of ceftriaxone administration, she developed sudden hypotension, tachycardia, pallor, and a hemoglobin drop from 11.9 g/dL to 7.1 g/dL, consistent with acute hemolysis.
This case shows that ceftriaxone induced DIIHA can cause abrupt, catastrophic hemolysis with rapid progression to DIC and death within hours, even in patients who previously tolerated the drug. Clinicians should suspect DIIHA in patients who develop sudden anemia, hemodynamic instability, or coagulopathy shortly after antibiotic exposure and promptly discontinue the suspected agent while coordinating urgent serologic evaluation. Greater awareness, systematic reporting, and further research are needed to refine diagnostic and management strategies.
-

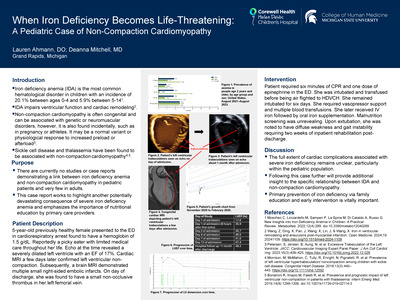
Race-Based Disparities in Advanced Heart Failure Evaluation and Outcomes
Anjali Purohit, Nabin Manandhar Shrestha, Michael Dickinson, David Fermin, Matthew Gonzalez, Ryan Grayburn, Milena Jani, Sangjin Lee, Eesha Purohit, and Renzo Loyaga-Rendon
Publication Date: 5-8-2026
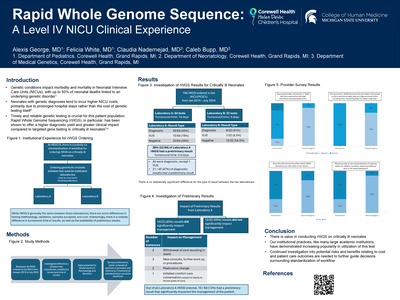
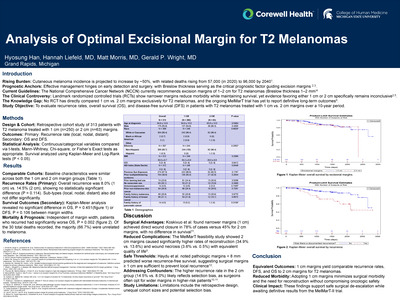
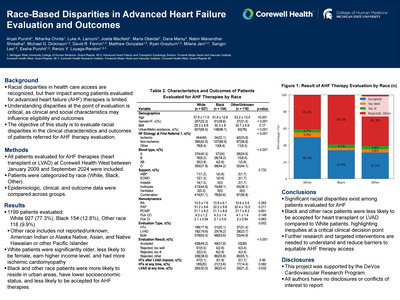
Racial disparities in access to health care have been described previously. However, limited data exist on how these disparities manifest in end stage heart failure patients at the time of evaluation for heart transplant or LVAD. The objective of this study is to evaluate racial disparities in the clinical characteristics and outcomes of patients referred for AHF therapy evaluation.
Racial disparities in access to health care have been described previously. However, limited data exist on how these disparities manifest in end stage heart failure patients at the time of evaluation for heart transplant or LVAD. The objective of this study is to evaluate racial disparities in the clinical characteristics and outcomes of patients referred for AHF therapy evaluation.
All patients evaluated for AHF therapies at Corewell Health West between January 2009 and September 2024 were included in this study. Patients were categorized by race into 3 groups (White, Black, other race). Epidemiologic, clinical, and outcome data were collected and compared across groups.
A total of 1199 patients were included in this study. Of these, 927 (77.3%) were White, 154 (12.8%) were Black, and 118 (9.9%) were other race. Significant differences were observed across groups (Table 1). In summary, White patients were older, less likely to be female, had a higher income level, and had more ischemic cardiomyopathy. Black and other race patients were more likely to reside in urban areas, have lower socioeconomic status, and less likely to be accepted for AHF therapies.
-

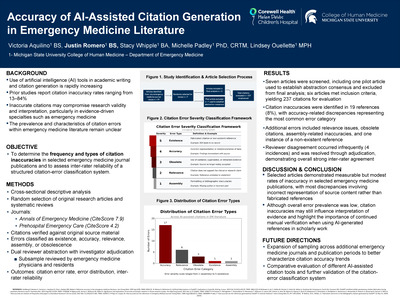
MI-SMART: A Consensus-Based Approach to Medical Clearance Before Inpatient Psychiatric Admission
Hailey Raab, Rayna Edwards, Juan Jimenez, Justin Romero, Hussein Kansou, Raine Johnson, Girish Sivakanthan, Andrea Ramirez, Tom Peterson, and Meredith Busman
Publication Date: 5-8-2026
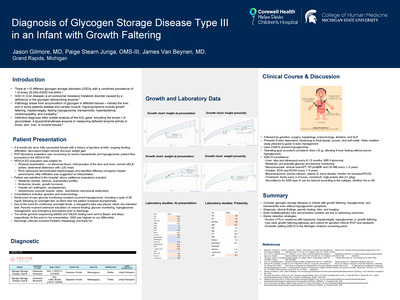
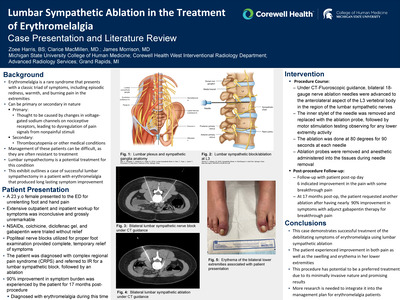
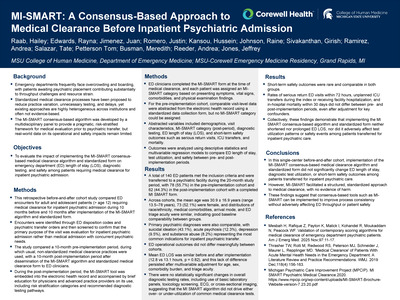
To evaluate the impact of implementing the MI-SMART consensus-based medical clearance algorithm and standardized form on emergency department (ED) length of stay (LOS), diagnostic testing, and safety among patients requiring medical clearance for inpatient psychiatric admission.
This retrospective before-and-after cohort study compared ED encounters for adult and adolescent patients (> 12 years of age) requiring medical clearance for inpatient psychiatric admission during 10 months before and 10 months after implementation of the MI-SMART algorithm and standardized form. Data abstracted included demographics, visit characteristics, MI-SMART category (post-period), diagnostic testing, ED length of stay (LOS), and short-term safety outcomes such as serious return visits, ICU transfers, and mortality. Outcomes will be analyzed using descriptive statistics and multivariable regression models to compare ED length of stay, test utilization, and safety between pre- and post-implementation periods.
A total of 140 ED patients met the inclusion criteria and were transferred to a psychiatric facility during the study period. Overall, 78 (55.7%) were in the pre-implementation cohort, and 62 (44.3%) were in the post-period with a completed MI-SMART form. The mean age was 30.9 + 16.9 years (range 13.5 to 78 years); 73 (52.1%) were female. Demographics, comorbidity, visit characteristics and psychiatric diagnoses were similar between the two cohorts. Common diagnoses were suicidal ideation (43.1%), acute psychosis (12.3%), depression (9.5%), and substance abuse (8.2%). ED LOS was similar between the two cohorts (12.8 vs. 13.1, p = 0.82). There were also no differences in test utilization or in short-term safety outcomes despite adjustment for key confounders.
Implementation of the MI-SMART consensus-based medical clearance algorithm and standardized form did not significantly change ED length of stay, diagnostic test utilization, or short-term safety outcomes among patients transferred for inpatient psychiatric care. However, MI-SMART facilitated a structured, standardized approach to medical clearance, with no evidence of harm. These findings suggest that consensus-based tools such as MI-SMART can be implemented to improve process consistency without adversely affecting ED throughput or patient safety.
-

A Case of Hydralazine Induced ANCA-Associated Vasculitis with Negative Anti-histone Antibodies
Bradley Reinoehl, Hannah Campbell, Gabriella Abreo, Jagroop Doad, Gabriel Tallent, and Kathleen Jarrett
Publication Date: 5-8-2026
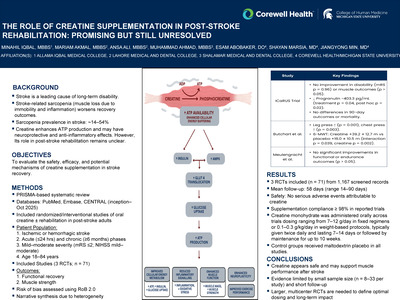
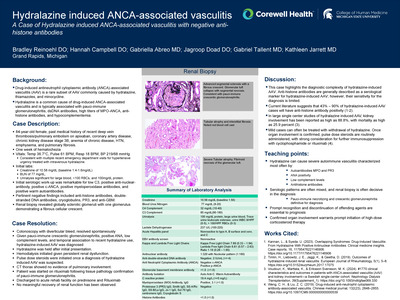
Drug-induced anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a rare subset of AAV commonly caused by hydralazine, thiamazoles, and minocycline. Hydralazine is a common cause of drug-induced ANCA-associated vasculitis and is typically associated with pauci-immune glomerulonephritis, dsDNA antibodies, high titers of MPO-ANCA, anti-histone antibodies, and hypocomplementemia.
An 84-year-old female with a past medical history of recent deep vein thrombosis/pulmonary embolism on apixaban, coronary artery disease, chronic kidney disease stage 3B and HTN presented with one week of hematochezia and was admitted for a subacute gastrointestinal bleed. She was found to be significantly hypertensive on arrival, consistent with multiple recent emergency department visits for hypertensive urgency treated with intravenous hydralazine. Initial workup was remarkable for a creatinine of 10.58 mg/dL (baseline 1.4-1.6mg/dL), BUN of 77 mg/dL, and urinalysis significant for large blood, >100 RBCs, and 100mg/dL protein. Initial serologic work-up was remarkable for low C3, positive anti-nuclear-antibody, positive c-ANCA, positive myeloperoxidase antibodies, and positive warm autoantibodies. Renal biopsy revealed globally sclerotic glomeruli with one glomerulus demonstrating an active cellular crescent. Anti-histone antibodies were found to be negative.
This case highlights the diagnostic complexity of hydralazine-induced AAV. Anti-histone antibodies are generally described as a serological marker for hydralazine-induced AAV; however, their sensitivity for the diagnosis is limited. Current literature suggests that 43% - 90% of hydralazine-induced AAV cases will have anti-histone antibody positivity. Without a distinctive marker for hydralazine-induced AAV, diagnosis relies on clinical acumen with a temporal exposure to hydralazine, serology data, and improvement of symptoms after medication cessation.
-

The Impact of Sternal Fractures in Patients with Blunt Thoracic Injury
Patrick Renner, Elizabeth Steensma, Laura Krech, Kyle Knapp, Kristen Hawes, Ashley Franklyn, and Giuseppe Zambito
Publication Date: 5-8-2026
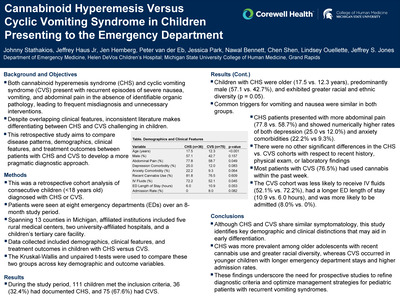
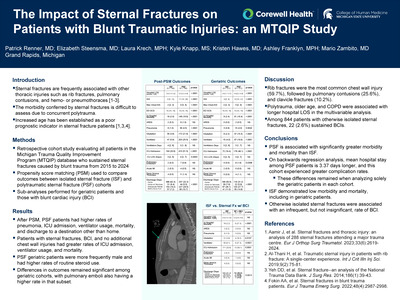
Traumatic sternal fractures present a clinical challenge to risk stratification and management strategies. An increasing burden of rib, clavicle, and scapula fractures with sternal injuries significantly increases adverse outcomes and mortality, although these risks have not been fully defined. Historically, the presence of sternal fractures has also evoked concern for underlying blunt cardiac injury (BCI), although no significant association with isolated sternal fractures has consistently been demonstrated. Therefore, knowledge gaps remain regarding the prognosis of sternal fractures with and without additional chest wall injuries, especially in the geriatric population. To further elucidate the impact of these injuries, this study aims to determine the morbidity conferred by isolated sternal fractures versus those with concurrent thoracic injuries.
This retrospective cohort study evaluated adult blunt trauma patients who sustained sternal fractures from 2015 to 2024. Qualifying patients were extracted from the Michigan Trauma Quality Improvement Program database, which houses information from the registries of 35 Level 1 and 2 trauma centers across the state. The primary outcome was hospital length of stay (LOS) between patients with isolated sternal fractures and those with additional chest wall injuries. Further sub-analysis of this outcome with a geriatric cohort was also performed. Secondary objectives included determination of differences in ventilator days, blunt cardiac injury, and adverse hospital events among these cohorts. Deidentified data was transferred to a statistician for extraction and analysis. Numeric outcomes were expressed as mean ± standard deviation. Propensity score matching (PSM) was used to compare isolated (ISF) and polytraumatic sternal fracture (PSF) cohorts. Significance was defined as p < 0.05.
822 patients had ISF, while 1,659 patients comprised the PSF cohort. The most commonly associated thoracic injury in the PSF cohort was rib fractures (59.7%), followed by pulmonary contusions (25.6%), clavicle fractures (10.2%), BCI (9.0%), and scapula fractures (2.5%). ISF patients were older and less frequently male. They had significantly higher rates of hypertension and steroid use, and a lower rate of tobacco abuse. After PSM, PSF patients had a significantly longer hospital LOS, which was 3.37 days longer than ISF patients (p< 0.0001). Additionally, the ISF cohort had significantly less in-hospital mortality, fewer ICU admissions, and lower rates of pneumonia, intubation, and ventilator usage. Among geriatric trauma patients, ISF patients were still less frequently male and more likely to use steroids routinely. After PSM, the geriatric PSF cohort had longer hospital LOS, greater in-hospital mortality, and higher rates of pneumonia, intubation, ventilator usage, ICU admission, and PE development.
In this retrospective study, we demonstrate that PSF is associated with significantly greater morbidity and mortality than ISF. The mean hospital stay among PSF patients is 3.37 days longer, and this cohort experienced greater rates of in-hospital mortality, ICU admission, pneumonia, intubation, and ventilator dependence. These significant differences remained when analyzing solely the geriatric patients in each cohort. Future studies should analyze the compounding effect of sternal fractures on patients with rib fractures.
-

A Diagnostic Sleight of Hand: Gallstone Ileus in a Busy Abdomen
Emily Ridge and Cathryn Chadwick
Publication Date: 5-8-2026
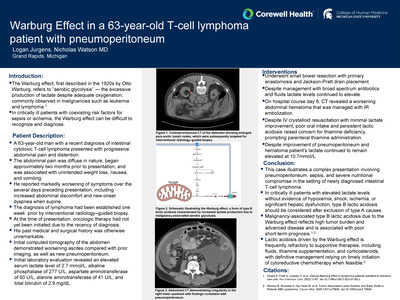
Gallstone ileus is a rare entity that occurs in only 0.3-0.5% of patients with cholecystitis and is the etiology of intestinal obstruction in less than 1% of cases. The infrequency with which it is encountered makes it a difficult diagnostic challenge, especially in the context of distracting radiologic findings.
76 year-old female initially presented with several days of diffuse abdominal pain, nausea, and vomiting. Initial ED workup at an OSH notable for WBC 15.8, Tbili 0.6, AST/ALT 16/13. CT A/P demonstrated a large choledochoduodenal fistula with pneumobilia, along with multiple dilated loops of small bowel, and a 2.6cm ovoid intraluminal mass just proximal to transition point in the right pelvis. As a result, the patient was subsequently transferred to Butterworth Hospital given the concern for a pathologic choledochoduodenal fistula necessitating hepatopancreatobiliary surgery expertise. Following transfer, additional history revealed that the patient had a past surgical history of open cholecystectomy with CBD exploration and choledochoduodenostomy and retained CBD stone that was unable to be removed at time of initial intervention, consistent with a post-surgical etiology of patient's CT findings.
Patient was subsequently admitted for small bowel obstruction management. Diagnostic laparoscopy converted to exploratory laparotomy revealed a 3cm gallstone in the mid jejunum for which an enterotomy with gallstone extraction was performed. Postoperatively, the patient had a complete recovery and was ultimately discharged home.
Gallstone ileus is an uncommon cause of presentation to the emergency department, representing less than 1% of small bowel obstruction cases. Here we present a case of gallstone ileus in a patient with abnormal radiographic findings, highlighting the importance of maintaining an understanding of surgical procedures that are becoming historical in order to aid in proper assessment and management, especially in patients who present with rare conditions.
-
: First Case at Our Institution by Emma Sand and Tina Wong-Gillam")
Implementing Laparoscopic Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC): First Case at Our Institution
Emma Sand and Tina Wong-Gillam
Publication Date: 5-8-2026
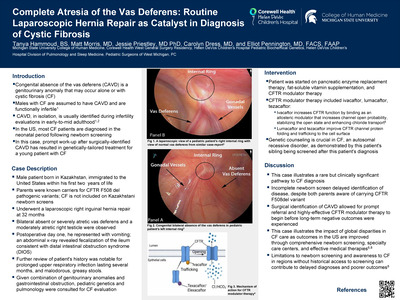
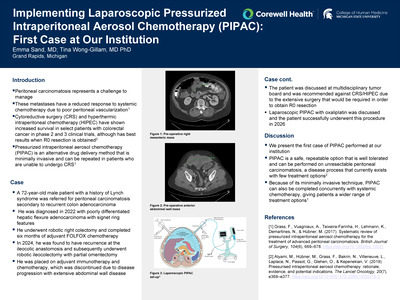
Peritoneal carcinomatosis represents a challenge to manage. These metastases have a reduced response to systemic chemotherapy due to poor peritoneal vascularization [1]. Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) have shown increased survival in select patients with colorectal cancer in phase 2 and 3 clinical trials, although has best results when R0 resection is obtained [2]. Pressurized intraperitoneal aerosol chemotherapy (PIPAC) is an alternative drug delivery method that is minimally invasive and can be repeated in patients who are unable to undergo CRS [1].
A 72 year-old male patient with a history of Lynch syndrome was referred for peritoneal carcinomatosis secondary to recurrent colon adenocarcinoma. He was diagnosed in 2022 with poorly differentiated hepatic flexure adenocarcinoma with signet ring features.
We present the first case of PIPAC performed at our institution. PIPAC is a safe, repeatable option that is well tolerated and can be performed on unresectable peritoneal carcinomatosis, a disease process that currently exists with few treatment options2. Because of its minimally invasive technique, PIPAC can also be completed concurrently with systemic chemotherapy, giving patients a wider range of treatment options [1].
-

Burkholderia Bedlam: A case of 'Cepacia syndrome' in a patient with Cystic Fibrosis
Vamsish Satoor
Publication Date: 5-8-2026
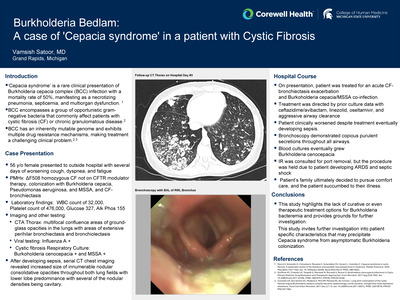
'Cepacia syndrome' is a rare clinical presentation of Burkholderia cepacia complex (BCC) infection with a mortality rate of 50%, manifesting as a necrotizing pneumonia progressing to septicemia and multiorgan dysfunction. Burkholderia cepacia complex encompasses a group of opportunistic gram-negative bacteria that most commonly affect patients with cystic fibrosis or chronic granulomatous disease. The airways of cystic fibrosis patients typically represent an evolving ecosystem forming a clonal population of any combination of Burkholderia species. BCC have an inherently very mutable genome and exhibit multiple drug resistance mechanisms. This coupled with variable drug resistance profiles make treatment of Burkholderia infection a very challenging clinical problem. The purpose of this investigation is to expose the lack of evidence on treatment options for Burkholderia infection.
I present a case of a 56 y/o female with PMHx of ΔF508 homozygous cystic fibrosis not on CFTR modulator therapy, colonization with Burkholderia cepacia, Pseudomonas aeruginosa, and MSSA, and CF-bronchiectasis who presented to outside hospital with several days of worsening cough, dyspnea, and fatigue. Initial evaluation revealed a WBC count of 32,000, platelet count of 476,000, glucose 327, and Alk Phos 155. CTA thorax showed multifocal confluence areas of ground-glass opacities in the lungs with areas of extensive perihilar bronchiectasis and bronchiolectasis. Viral testing returned positive for Influenza A. A cystic fibrosis respiratory culture demonstrated infection with Burkoholderia cenocepacia and MSSA. After patient developed sepsis in the hospital, serial CT chest imaging revealed significantly increased size and number of innumerable nodular consolidative opacities throughout both lung fields with lower lobe predominance with several of the nodular densities being cavitary.
Overall, this study highlights the lack of curative or even therapeutic treatment options for Burkholderia bacteremia and provides grounds for further investigation. Additionally, this study invites further investigation into patient specific characteristics such as viral infection, long-term central venous access, and lack of disease modifying therapy that may precipitate cepacia syndrome from asymptomatic Burkholderia colonization. Identifying risk factors for the development of cepacia syndrome may allow for more aggressive treatment of predisposed patients.
-

From Palliation to Possibility: 3D Modeling Guided Biventricular Conversion and Subsequent PAPVR Repair in a Complex Congenital Heart Disease
Asmita Sharma, Tayaba Miah, and Marcus Haw
Publication Date: 5-8-2026
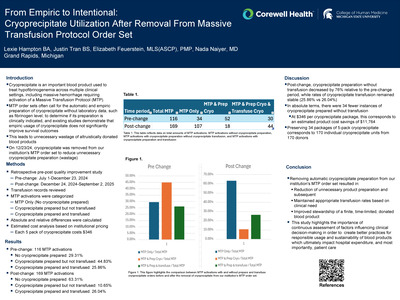
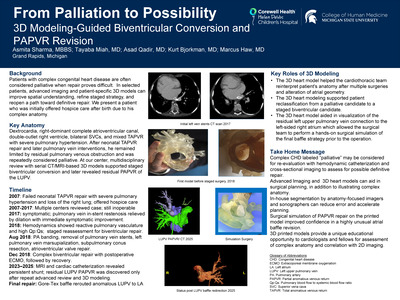
Three-dimensional cardiac modeling and printing are increasingly used in complex congenital cardiac surgery to help define the anatomy and spatial relationships and support more confident surgical planning. We report a child with heterotaxy, dextrocardia, right-dominant complete atrioventricular canal, double outlet right ventricle, and mixed total anomalous pulmonary venous return who had been repeatedly classified as inoperable and palliative. At our institution, an in-house multidisciplinary 3D modeling team enabled rapid segmentation of high-resolution CT/MRI data, creation of patient-specific printed heart models, and hands-on rehearsal of staged biventricular repair strategies. These models clarified intricate anatomical relationships, guided initial pulmonary venous reconstruction and intracardiac baffling, and later helped identify a plausible explanation for a residual partial an
The evolution of advanced cross-sectional imaging with CT and MRI, combined with interactive visualization and 3D printing of accurate models, has allowed experienced teams to consider repairs in cases where previously it was felt impossible.
This case supports the growing evidence that 3D cardiac modeling can offer new hope to patients labeled palliative by revealing repair pathways that are not apparent on traditional imaging alone and highlights importance of revisiting diagnoses deemed inoperable as we continue to make strides in advanced imaging and 3D simulations.
-

Posterior Reversible Encephalopathy Syndrome Following Donanemab Infusion: A Novel Adverse Effect in Alzheimer's Disease Therapy
Aldo Shehaj, Naser HajAissa, Mary M. Mcphail Ciufo, and Jiangyong Min
Publication Date: 5-8-2026
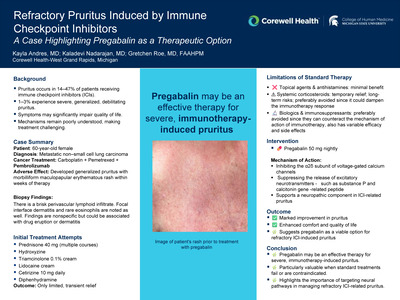
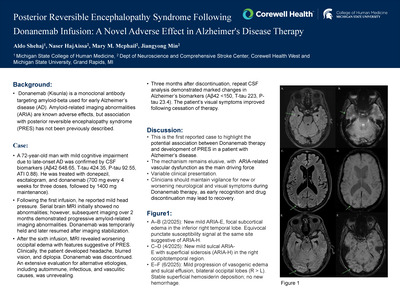
Background: Donanemab (Kisunla) is a monoclonal antibody targeting amyloid-beta used for early Alzheimer's disease (AD). Amyloid-related imaging abnormalities (ARIA) are known adverse effects, but association with posterior reversible encephalopathy syndrome (PRES) has not been previously described.
A 72-year-old right-handed man with mild OSA, IBS, asthma, and hyperlipidemia was followed for progressive memory loss since age 66, consistent with mild cognitive impairment due to late-onset Alzheimer's disease. CSF AD biomarkers (Aβ42 648.65, T-tau 424.35, P-tau 92.55, ATI 0.88) confirmed the diagnosis.
This case highlights a potential association between Donanemab therapy and development of PRES in a patient with Alzheimer's disease, possibly mediated by severe ARIA-related vascular dysfunction. Clinicians should maintain vigilance for new or worsening neurological and visual symptoms during Donanemab therapy, as early recognition and drug discontinuation may lead to recovery.
-

Effects of Medical Students and Family Medicine Trainees/Educators' Attitudes and Knowledge About Disability on Clinical Decision-Making
Christine Skovira, Roksolana Sudyk, Matthew Almany, Harland Holman, Laura VanPuymbrouck, Ariel Cascio, Nishika Patel, Simran Bhogal, and Rachelle Pichot
Publication Date: 5-8-2026
One in four adults in the United States live with a disability, with mobility impairments affecting 14%. Persons with disabilities (PWD) consistently receive less preventive care and experience poorer health outcomes. Contributing factors include provider attitudes, limited training, and low awareness. This study examined whether medical trainees', and family medicine residents/educators, perceptions of PWD influence clinical decision-making.
An anonymous survey was distributed to medical students, family medicine residents and family medicine educators. Respondents reviewed a clinical case involving acute low back pain and hypertension and were randomly assigned to a patient with (CASE A) or without (CASE B) a mobility disability (lower limb amputation). They then answered multiple-choice and free-response questions on management decisions. Descriptive statistics and frequency tables summarized data.
A total of 118 medical students (years 1-4) and 28 family residents/faculty were surveyed for a total of 146 respondents. Demographics included training level, gender, disability status, and family history of mobility disability. Quantitative and qualitative analysis is currently being performed on the dataset. Quantitative analysis looks to compare responses to multiple choice questions between case A and B. Preliminary results of quantitative data does not show much clinical significance between responses. Our statistician is currently writing up a summary of the most interesting non-statistically significant results. In regards to the quantitative data (free response questions), we are currently analyzing the data using a systematic inductive coding approach designed to classify clinical reasoning into quantifiable categories suitable for mixed-methods analysis.
This is the first case-based study to examine how medical students' and family medicine trainees/educators perceptions of PWD relate to clinical decision-making. Preliminary findings suggest that disability bias may NOT influence clinical decision making in PWD (these findings refute our hypothesis). Despite the fact, medical curricula should continue to address how stigma and misconceptions about disability shape care delivery. Additional studies, with larger sample sizes, may be needed to support our findings.
-

More Than Just a Rash: A Case of Neonatal Lupus Syndrome Uncovering Maternal Autoimmunity
Rebecca Smith, Sonia Gentile, Abeba Berhane, and Katherine Foster
Publication Date: 5-8-2026
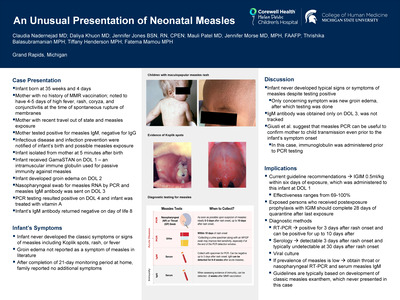
Neonatal lupus syndrome (NLS) is a rare immune-mediated condition that results from the passive transfer of maternal autoantibodies to the fetus. Autoantibodies known to cause NLS include Sjogren (anti-SSA and anti-SSB) and anti-U1-ribonucleoprotein immunoglobulin G (IgG) antibodies. These antibodies are typically seen in association with maternal systemic lupus erythematosus (SLE), Sjogren's syndrome, rheumatoid arthritis, and other systemic autoimmune conditions. Fetuses and newborns born to women with known rheumatologic disease and seropositivity for high-risk antibodies are monitored closely for clinical manifestations of NLS. However, a subset of newborns diagnosed are born to women with no previous diagnosis of autoimmune disease. Here, we report a case of a newborn who presented with a leading to the diagnosis of both infantile and maternal autoimmune disease.
A 2-week-old male born at 36 weeks presented for a routine well-child exam with maternal concern about a facial rash that had been present since approximately one week of life. On examination, he had multiple annular, raised erythematous patches with central clearing on his face. Over the following weeks, these lesions gradually expanded and coalesced, and new lesions appeared on his face, limbs, and trunk. His mother underwent laboratory evaluation revealing positive ANA at 1:1280 titer, as well as positive anti-SSA and SSB antibodies, confirming the diagnosis of NLS. Further evaluation of the infant with EKG and echocardiogram did not reveal any evidence of congenital heart block or other cardiac manifestations of NLS. His rash resolved spontaneously by six months of age.
Neonates presenting with a classic rash or congenital heart block should be evaluated for neonatal lupus syndrome. The absence of known maternal rheumatologic disease does not preclude a diagnosis of neonatal lupus syndrome and mothers of these infants should be monitored closely for development of rheumatologic disease.
-

Improving Educational Outcomes in Rural General Surgery Rotations: A Quality Improvement Initiative
Doug Snow
Publication Date: 5-8-2026
Access to high-quality surgical care in rural and resource-limited settings remains a persistent challenge in the United States, largely driven by disparities in the distribution of the general surgery workforce. Rural communities experience disproportionate shortages of surgeons, contributing to delays in care and limited access to essential surgical services. In recognition of this need, graduate medical education has increasingly emphasized exposure to rural practice environments, with recent Accreditation Council for Graduate Medical Education requirements encouraging training in resource-limited settings. In 2023, the Corewell Health West General Surgery Residency Program implemented a postgraduate year (PGY)-3 rural general surgery rotation at Pennock Regional Hospital in Hastings, Michigan. The rotation was designed to provide broad clinical exposure, increased operative autonomy,
This quality improvement initiative evaluated a postgraduate year (PGY)-3 rural general surgery rotation at Pennock Regional Hospital in Hastings, Michigan, within the Corewell Health West General Surgery Residency Program. All residents who completed the rotation were eligible to participate. A voluntary, anonymous survey was distributed via Microsoft Forms following rotation completion. No personal identifiers were collected, and responses were de-identified at submission. The survey included Likert-scale and open-ended items assessing educational content, operative autonomy, case mix, faculty engagement, logistics, and overall satisfaction. Quantitative data were analyzed using descriptive statistics, including proportions and central tendency measures. Qualitative responses underwent inductive thematic analysis by independent reviewers to identify recurrent themes and actionable feedback. Data were securely stored and accessed only by the approved project team. Findings were review
Nine PGY-3 residents completed the survey (100% response rate). Overall satisfaction with the rural rotation was high. Most residents agreed or strongly agreed that they were exposed to an appropriate breadth of general surgical cases (77.8%) and that operative volume was suitable for their training level (77.8%). Increased operative autonomy was reported by 66.7% of respondents, while 88.9% agreed that faculty provided effective supervision and teaching. All respondents agreed that the rotation contributed positively to their residency education, and 88.9% stated they would recommend the rotation to other residents. Exposure to resource-limited practice environments and multidisciplinary collaboration was consistently reported as beneficial. Fewer residents indicated that the rotation influenced their long-term career interest toward rural or community practice (44.4%). Qualitative analysis identified operative autonomy, exposure to advanced endoscopy and robotic surgery, and insight into rural healthcare sys
The PGY-3 rural general surgery rotation provided meaningful educational value and was highly rated by participating residents. The rotation offered appropriate operative autonomy, strong faculty engagement, and valuable exposure to rural surgical practice. While its influence on career choice was variable, resident feedback supports continued incorporation of structured rural rotations. Ongoing evaluation and targeted refinements may further enhance the educational impact and sustainability of rural surgical training experiences.
-

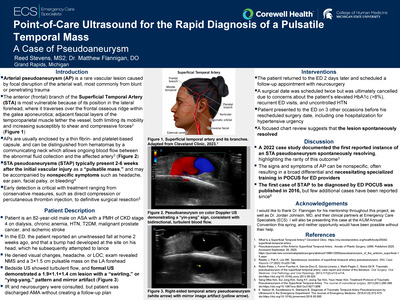
Point-of-Care Ultrasound for the Rapid Diagnosis of a Pulsatile Temporal Mass: A Case of Pseudoaneurysm
Reed Stevens and Matthew Flannigan
Publication Date: 5-8-2026
-

Double Trouble! Concomitant PML and Neurosyphilis Infection in Patient with Progressive Dysarthria with History of CVA and AIDS: A Case Report
Emma Streveler, Ryan Crane, Hannah Bray, Talawnda Bragg, and Gordana Simeunovic
Publication Date: 5-8-2026
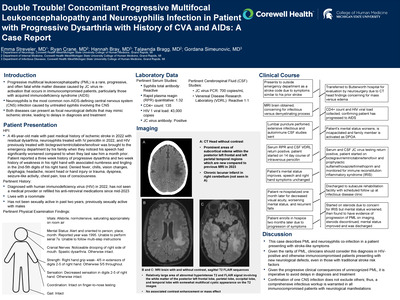
Progressive multifocal leukoencephalopathy (PML) is a rare, progressive, and often fatal, white matter disease caused by JC virus re-activation that occurs in immunocompromised patients, particularly those with AIDS. Neurosyphilis is the most common non-AIDS-defining central nervous system (CNS) infection caused by untreated syphilis involving the CNS. Both diseases can present as focal neurologic deficits that may mimic ischemic stroke, making it difficult to identify upon presentation, even in patients who are immunocomprised. We report a case of PML and neurosyphilis coinfection in a patient with prior ischemic stroke with known residual dysarthria, who presented to the hospital as a stroke code activation.
49-year-old male with past medical history of HIV/AIDs not on any antiretroviral therapy, and prior ischemic stroke with residual dysarthria presented to the emergency department for acute worsening of his dysarthria and new paresthesia. A stroke code was activated. A non-contrast CT head revealed subcortical edema in the posterior left frontal and left parietal temporal regions. Brain MRI demonstrated T2 FLAIR hyperintensities within these regions consistent with white matter disease. Blood work showed a CD4+ count of 135 cells/uL, viral load 43000 copies/mL, and serum RPR 1:32. Cerebrospinal fluid testing revealed JC virus level of 700 copies/ml and VDRL 1:1.
Given the rarity of PML, clinicians should consider this diagnosis in HIV-positive patients presenting with new neurological deficits, even in those with traditional stroke risk factors, to avoid delays in antiretroviral therapy initiation. Furthermore, confirmation of one CNS infection does not exclude others, a comprehensive CNS infectious workup is warranted in all HIV-positive patients with neurological manifestations.
-

Unexpected Pancreatic Duplication Cyst
Allison Swider-Ebels, Kristen Hawes, and Elliot Pennington
Publication Date: 5-8-2026
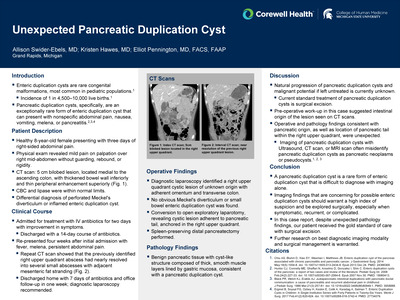
Enteric duplication cysts are rare congenital malformations, most often occurring in pediatric populations with an incidence of 1 in 4,500-10,000 live births. Pancreatic duplication cysts are an even rarer form of enteric duplication cysts. Presenting symptoms are nonspecific abdominal pain, nausea, melena or pancreatitis. Initial imaging is typically ultrasound, CT, or MRI, which often misidentify these as pancreatic neoplasms or pancreatic pseudocysts. The current standard of treatment for pancreatic duplication cysts is surgical excision.
An otherwise healthy 8-year-old female presented with three days of right-sided abdominal pain and diarrhea. CT scan showed a 5 cm bilobed lesion, located medial to the ascending colon, with thickened bowel wall inferiorly and thin peripheral enhancement superiorly. Laboratory findings, including complete blood count and lipase, were within normal limits. On physical exam, there was mild pain localized over the right mid-abdomen. The leading differential diagnosis was perforated Meckel's diverticulitis or inflamed enteric duplication cyst. Treatment consisted of antibiotics for 14 days. After completion of the antibiotic course, the patient returned with fevers, melena, and continued abdominal pain. Repeat CT scan showed near resolution of the previously identified lesion with continued surrounding inflammation. Due to persistent symptoms and concern for recurrence, the decision was made to proceed to the operating room for a diagnostic laparoscopy.
Pancreatic duplication cysts are rare and difficult to diagnose. This particular case was unique since preoperative work-up did not suggest pancreatic origin of the lesion, but rather favored an intestinal source. Due to the unknown natural progression or malignant potential of untreated pancreatic duplication cysts, surgical intervention for imaging findings that are concerning for enteric duplication cysts should be pursued when symptomatic, recurrent, or complicated. Further research on the best diagnostic imaging modality and surgical removal is warranted.
-

Maternal Autonomy and Refusal of Medically Advised Cesarean Delivery
Derek Tonello, Laura Lyons, and Matthew Armstrong
Publication Date: 5-8-2026
Repeated cesarean section (CS) refusal creates ethical challenges for healthcare teams. Patient autonomy must be balanced with preparedness for emergent maternal or fetal compromise. High-risk pregnancies typically involve an interdisciplinary team including obstetricians or maternal-fetal medicine specialists, nurses, obstetric anesthesiologists, and neonatology as indicated. Ethics consultants, social work, and additional support staff are involved depending on maternal or fetal risk factors.
A 35 year old G11P9 female with an ongoing pregnancy was indicated for CS. The patient's pregnancy was high-risk due to 3 CSs, 5 VBACs, a history of preterm labor and delivery in 3 pregnancies. The patient refused CS and other advised treatments in her previous four pregnancies. The current pregnancy was complicated by anemia and a fetal right aortic arch defect. The patient was adamant about CS refusal, even in the event that her and her child would otherwise die. The patient was DNR status and designated a DPOA. She also refused recommended therapies such Rhogam, neonatal vaccinations, blood transfusions, and vitals/fetal monitoring. Many discussions were had between providers and the patient about the implication of her decisions and her understanding of them. The patient had a history of discord with healthcare providers and potential psychiatric concerns, including a suicide attempt. A psychiatric consult was suggested during this pregnancy but the patient refused.
This case illustrates the challenges of balancing optimal medical practices with patient autonomy. Many ethical challenges arise when patients refuse indicated care. These are further complicated by pregnancy, in which there is concern for both the mother and the child. This medical team handled them by ensuring patient understanding, involving an interdisciplinary team, and striving to administer the best care while respecting patient autonomy. A good understanding of these challenges is critical for achieving better outcomes when patients refuse medical treatments.
-

Bronchobiliary Fistula Following Radioembolization Managed with IR‑Guided Drainage: A Case Report
Abigail Townley, Dylan Goldsmith, and William Slater
Publication Date: 5-8-2026
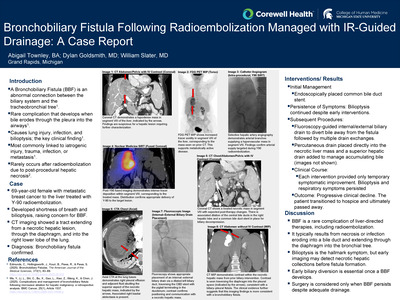
A Bronchobiliary Fistula (BBF) is a pathological communication between the biliary system and the tracheobronchial tree. This communication is due to a rare complication that results from a bile collection eroding through the pleura and into the small airways. The resulting destruction of lung tissue can lead to chronic infections as well as bilioptysis, the presence of bile in the sputum, a defining feature of BBF. BBFs are most associated with iatrogenic injury, trauma, infection, and metastasis. Rarely, Radioembolization and subsequent post-procedural necrosis may create conditions for BBF formation.
A 69-year-old female with a history of breast cancer metastatic to the liver was treated with radioembolization (Y-90). She later presented with shortness of breath accompanied by bilioptysis, leading to suspicions of BBF. CT demonstrated a tract extending from the necrotic liver mass, through the diaphragm, and into the right lower lobe of the lung.
BBF is a rare complication of radioembolization, forming when tissue necrosis/infection erodes into an adjacent bile duct, and then through the diaphragm into the bronchial tree. Interventional radiologists should recognize this potential complication in patients undergoing liver‑directed therapies. While bilioptysis is the key symptom, cross‑sectional imaging can detect a necrotic/infected hepatic collection earlier, allowing intervention that may prevent BBF. Once a BBF occurs, early biliary diversion is imperative, with surgery usually reserved for persistent cases.
-

PACU Recurarization: The Challenges of Reversing Rocuronium with Sugammadex
Peter van der Eb, Sydney Musick, and Nicholas Watson
Publication Date: 5-8-2026
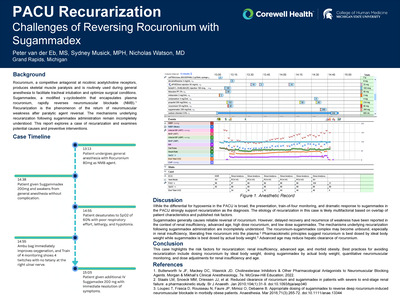
Rocuronium, a competitive antagonist at nicotinic acetylcholine receptors, produces skeletal muscle paralysis and is routinely used during general anesthesia to facilitate tracheal intubation and optimize surgical conditions. Sugammadex, a modified γ-cyclodextrin that encapsulates plasma rocuronium, rapidly reverses neuromuscular blockade. Recurarization is the phenomenon of the return of neuromuscular weakness after paralytic agent reversal. The mechanisms underlying recurarization following sugammadex administration remain incompletely understood. This report explores a case of recurarization and examines potential causes and preventive interventions.
A 72 yo woman presented for CT-guided kidney ablation for renal cell carcinoma. PMH was significant for morbid obesity (111.1 kg), asthma, and chronic renal insufficiency. The procedure and general anesthetic were unremarkable. The patient received rocuronium 80 mg which was reversed with sugammadex 200 mg 85 minutes later. She was stable in the post-anesthesia care unit (PACU) for 15 minutes until she complained of shortness of breath followed by acute oxygen desaturation and poor respiratory effort. Bag-valve-mask ventilation improved oxygenation. She appeared "floppy" and was unable to raise arms or legs to command. Train-of-four monitoring at the ulnar nerve demonstrated four twitches without tetany. Sugammadex 200 mg was administered followed by immediate resolution of muscle weakness. When she was interviewed after stabilization, she described the anxiety of being unable to speak, breath, or move despite being awake and alert throughout.
This case highlights the risk factors for recurarization: renal insufficiency, advanced age, and obesity. Best practices for avoiding recurarization include dosing rocuronium by ideal body weight, dosing sugammadex by actual body weight, quantitative neuromuscular monitoring, and dose adjustments for renal insufficiency and age.
-

Creating Effective Influenza Vaccine Patient Education Materials
Jensen Vickerman and Angela Oosterman
Publication Date: 5-8-2026
Influenza vaccination rates continue to fall below public health goals in the United States; however, the beliefs that influence influenza vaccine hesitancy among patients who receive other vaccines remain insufficiently addressed in primary care patient education.
Here, a literature search was conducted using the Center for Disease Control and Prevention and PubMed resources to develop an easy to provide education material for physicians that addresses common reasons for vaccine refusal, considerations for population health literacy and optimized presentation of information to encourage vaccination. Search terms included "influenza safety", "influenza mortality" and "effective patient education".
Common reasons for influenza vaccine refusal included lack of trust in vaccine safety, belief that the vaccine is ineffective, inadequate education regarding the severity of the flu and the perception that vaccines are politically motivated. Patient education materials effectiveness were linked to their brevity, visual appeal and focus on one clear main idea. Universal health literacy precautions emphasized presenting information in small, concrete steps and avoiding medical jargon when possible.
Influenza continues to contribute to preventable mortality in the United States each year. Despite the proven effectiveness of the influenza vaccine, vaccination rates continue to decline. For these reasons, it is important to continue to utilize and further develop patient education materials to better inform the public about the importance of influenza vaccination.
-

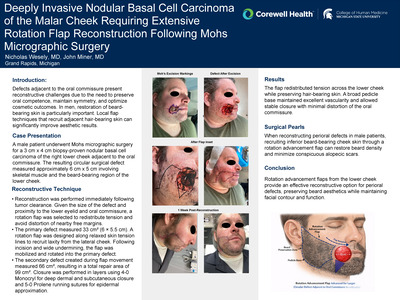
Peri-oral Reconstruction Following Mohs Surgery: An Aesthetic Consideration with Hair-bearing Skin
Nicholas Wesely and John Miner
Publication Date: 5-8-2026
-

Fournier's Gangrene in the Emergency Department: Insights from an Age-Stratified Population
Natalie Woodland, Aleezay Khan, Sydney Hudock, Emily Hill, Jon Giolitti, Kimberly Forman, Rachelle Pichot, Matthew Hysell, Matthew Singh, and Jason Seamon
Publication Date: 5-8-2026
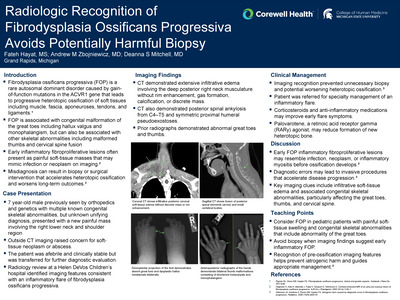
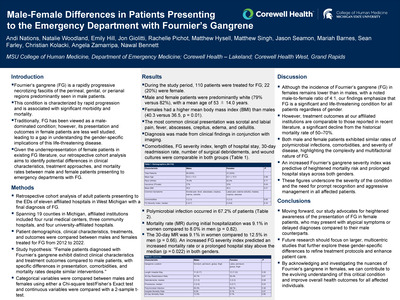
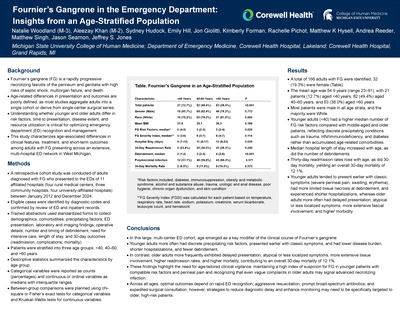
Fournier's gangrene (FG) is a rapidly progressive necrotizing fasciitis of the perineum and genitalia. Age-related differences in FG presentation and morbidity remain poorly defined. This study evaluated clinical characteristics, management strategies, and complications by age among adults diagnosed with FG in emergency departments (EDs).
A retrospective cohort study was conducted of all adults presenting to the EDs of 11 hospitals in West Michigan with FG from 2012 to 2024. Institutions included rural, community, and university-affiliated hospitals across 19 counties. Demographics, clinical features, treatments, and outcomes were extracted and compared by decade of age. Categorical variables were analyzed using Chi-square or Fisher's exact test; continuous variables with a two-sample t-test.
During the study period, 166 patients were treated for FG; 19.3% were female. Patients were predominantly white (78% males, 82% females); the mean age was 54.9 years (range, 23-91 years). FG among young adults (< 40) was diagnosed in 21 patients (12.7%) and was associated with trauma, HIV, immunodeficiency, or diabetes, often with rapid onset and classic symptoms prompting early admission. In 35.5% of those under age 50, tissue necrosis was limited unless the diagnosis was delayed or the patient was immunocompromised. Hospital stays were shorter, and fewer repeat debridement were required for patients over age 50. Older adults (>60) more often had extensive necrosis, atypical symptoms, and delayed admission. Overall, 30-day mortality was 12.1%.
Fournier's gangrene in younger adults is typically precipitated by trauma, immunodeficiency, or diabetes, and tends to present rapidly with classic symptoms, resulting in less extensive disease and better outcomes than older adults. In contrast, older patients are more likely to have delayed and atypical presentations, extensive tissue involvement, and higher morbidity. These results underscore the importance of age-specific clinical vigilance and prompt management to optimize outcomes in FG.
-

Lyme Carditis Leading to Ventricular Tachycardia
Zachary Yono, Lucas Rich, and Sinan Tankut
Publication Date: 5-8-2026
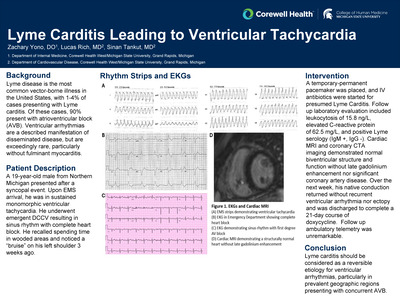
Lyme disease is the most common vector-borne illness in the United States, with 1-4% of cases presenting with Lyme carditis. Of these cases, 90% of patients present with atrioventricular block (AVB). Ventricular arrhythmias are a described manifestation of disseminated disease, but are exceedingly rare, particularly without evidence of fulminant myocarditis.
A 19-year-old male from Northern Michigan presented after suffering a syncopal event. Upon EMS arrival, he was in sustained monomorphic ventricular tachycardia. He underwent an emergent DCCV resulting in sinus rhythm with complete heart block. He recalled spending time in wooded areas and noticed a "bruise" on his left shoulder 3 weeks ago.
Lyme carditis should be considered as a reversible etiology for ventricular arrhythmias, particularly in prevalent geographic regions presenting with concurrent AVB.
-
 triggered by Febrile Ulceronecrotic Mucha-Habermann Disease (FUMHD): A Case Report. by Syed Zia, Sohail Qadir, Aryaan Khan, and Mauli Patel")
An Uncommon Presentation of Hemophagocytic Lymphohistiocytosis (HLH) triggered by Febrile Ulceronecrotic Mucha-Habermann Disease (FUMHD): A Case Report.
Syed Zia, Sohail Qadir, Aryaan Khan, and Mauli Patel
Publication Date: 5-8-2026
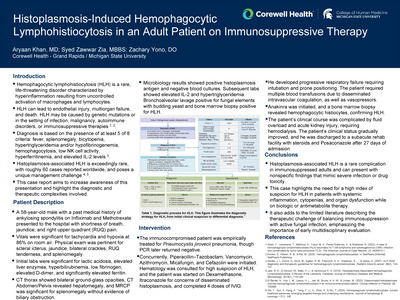
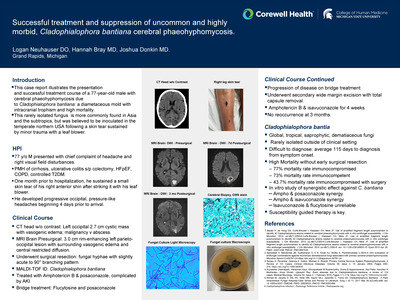
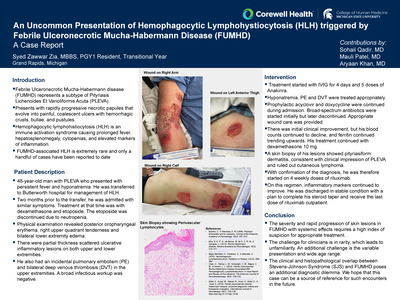
Pityriasis lichenoides et varioliformis acuta (PLEVA) is a group of inflammatory skin disorders. Febrile Ulceronecrotic Mucha-Habermann disease (FUMHD) represents a subtype with rapidly progressive necrotic papules that evolve into painful, coalescent ulcers with hemorrhagic crusts, bullae, and pustules [1]. Systemic manifestations include high fever, sore throat, diarrhea, central nervous system symptoms, abdominal pain, interstitial pneumonitis, splenomegaly, arthritis, sepsis, megaloblastic anemia, conjunctival ulcers, and death [2]. Hemophagocytic lymphohistiocytosis (HLH) is an immune activation syndrome causing prolonged fever, hepatosplenomegaly, cytopenias, and elevated markers of inflammation [3]. FUMHD-associated HLH is extremely rare and only a handful of cases have been reported to date [4]. This is a case of an HLH flare triggered by underlying FUMHD.
The patient is a 48-year-old man with PLEVA who presented with persistent fever and hyponatremia. He was transferred to Butterworth hospital in Grand Rapids, Michigan for management of HLH. Two months prior to the transfer, he was admitted with similar symptoms and met HLH criteria. At the time, treatment was started with dexamethasone and etoposide. The etoposide was discontinued due to neutropenia. At the time of admission, he had fatigue and lethargy but was alert and oriented. Vital signs were unremarkable except for fever and tachycardia. Physical examination revealed posterior oropharyngeal erythema, right upper quadrant tenderness and bilateral lower extremity edema. There were partial thickness scattered ulcerative inflammatory lesions on both upper and lower extremities. He also had an incidental pulmonary embolism (PE) and bilateral deep venous thrombosis (DVT) in the upper extremities. A broad infectious workup was negative.
The severity and rapid progression of skin lesions in FUMHD with systemic effects requires a high index of suspicion for appropriate treatment. The challenge for clinicians is in rarity, which leads to unfamiliarity. An additional challenge is the variable presentation and wide age range. The clinical and histopathological overlap between Stevens-Johnson Syndrome (SJS) and FUMHD poses an additional diagnostic dilemma [5]. We hope that this case can be a source of reference for such encounters in the future.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.