


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-

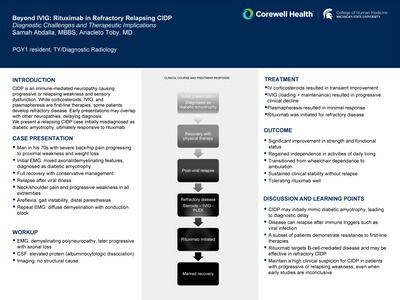
Mpox-Induced Proctitis: Diagnostic Uncertainty in a Patient with Previously Untreated HIV Infection
Denise Dawley, Matt Morris, Jessica Wassef, and James Ogilvie Jr.
Publication Date: 5-8-2026
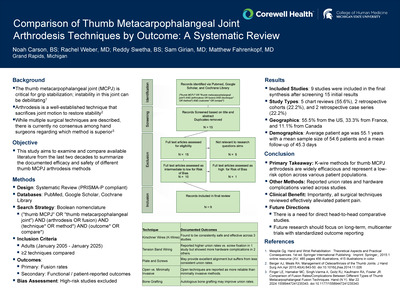
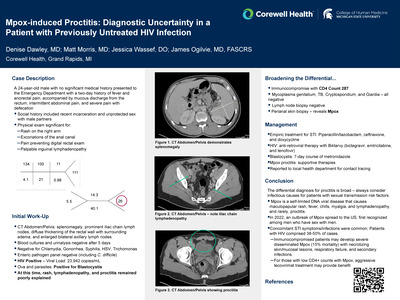
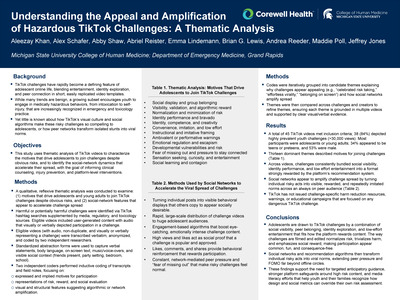
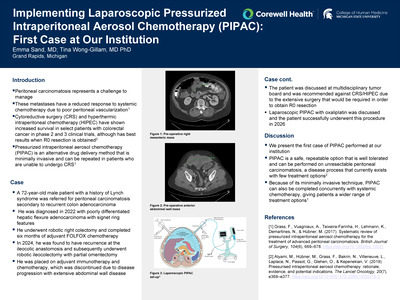
The World Health Organization describes mpox (formerly monkeypox) as a self-limited rash illness, typically presenting with nonspecific symptoms such as fever, muscle aches, and swollen lymph nodes. Historically, zoonotic mpox infections were recognized by distinctive rashes appearing on the face, palms, and soles of the feet. However, the multicountry outbreak in 2022 revealed atypical manifestations of mpox, including the development of proctitis in approximately 30% of patients, most of whom were men who have sex with men.
A 24-year-old male with no notable medical history presented with a two-day history of fever and anorectal pain, accompanied by mucous discharge from the rectum, intermittent abdominal pain, and severe pain with defecation. Significant social history factors included unprotected sex with men and recent incarceration. On physical examination, a rash was observed on the right arm, along with excoriations of the anal canal, which prevented a bedside digital rectal exam. Palpable inguinal lymphadenopathy was also noted. Imaging studies revealed splenomegaly, numerous prominent iliac chain lymph nodes, diffuse thickening of the rectal wall with surrounding edema, and enlarged bilateral axillary lymph nodes. Laboratory evaluation showed a positive HIV viral load and a CD4 count of 287, as well as a positive stool for Blastocystis test. Biopsies from the rash and perianal region were gathered during hospital stay, but results were not available until after discharge.
Though uncommon, mpox-induced proctitis should be considered in differential diagnoses for patients with sexual transmission risk factors. In the 2022 outbreak, concomitant STI were common, and HIV patients comprised 38-50% of cases.[2,3] Aggressive treatment with tecovirimat may benefit immunocompromised patients with low CD4+ counts who can develop severe disseminated mpox, resulting in necrotizing skin lesions, respiratory failure, and death.
-

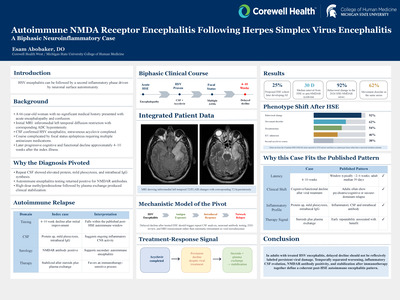
Admission Patterns and Clinical Outcomes in a Regional Cohort of Low-Intermediate Risk Pulmonary Embolism Patients
Larissa Dean, Justin Romero, John Oostema, and Joshua Reynolds
Publication Date: 5-8-2026
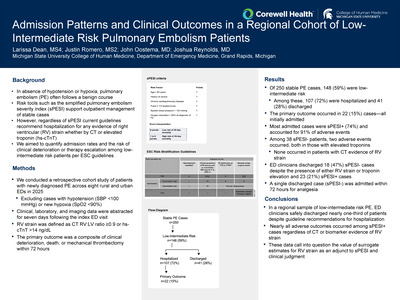
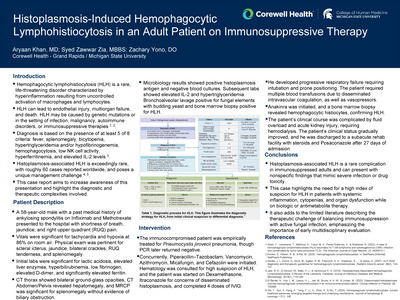
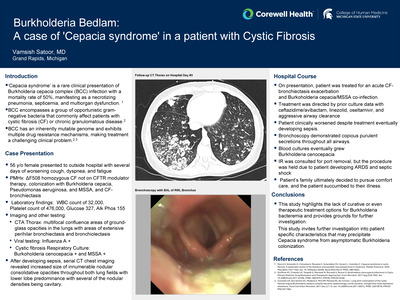
In the absence of hypotension or hypoxia, pulmonary embolism (PE) often follows a benign course. Risk tools such as the simplified pulmonary embolism severity index (sPESI) support outpatient management of stable cases; however, current guidelines recommend hospitalization for any evidence of right ventricular (RV) strain-whether by CT or elevated troponin (hs-cTnT)-regardless of sPESI. We aimed to quantify admission rates and the risk of clinical deterioration or therapy escalation among low-intermediate risk patients per ESC guidelines.
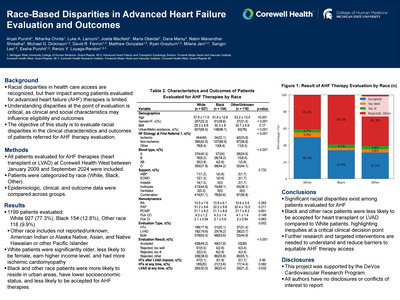
We conducted a retrospective cohort study of patients with newly diagnosed PE across eight rural and urban EDs in 2025, excluding cases with hypotension (SBP < 100 mmHg) or new hypoxia (SpO₂ < 90%). Clinical, laboratory, and imaging data were abstracted for seven days following the index ED visit. RV strain was defined as CT RV:LV ratio ≥0.9 or hs-cTnT >14 ng/dL. The primary outcome was a composite of clinical deterioration, death, or mechanical thrombectomy within 72 hours.
Of 250 stable PE cases, 148 (59%) were low-intermediate risk. Among these, 107 (72%) were hospitalized and 41 (28%) discharged. The primary outcome occurred in 22 (15%) cases-all initially admitted. Most admitted cases were sPESI+ (74%) and accounted for 91% of adverse events. Among 38 sPESI- patients, two adverse events occurred, both in those with elevated troponins; none occurred in patients with CT evidence of RV strain. ED clinicians discharged 18 (47%) sPESI- cases despite the presence of either RV strain or troponin elevation and 23 (21%) sPESI+ cases. A single discharged case (sPESI-) was admitted within 72 hours for analgesia.
In a regional sample of low-intermediate risk PE, ED clinicians safely discharged nearly one-third of patients despite guideline recommendations for hospitalization. Nearly all adverse outcomes occurred among sPESI+ cases regardless of CT or biomarker evidence of RV strain. These data suggest call into question the value of surrogate estimates for RV strain as an adjunct to sPESI and clinical judgment.
-

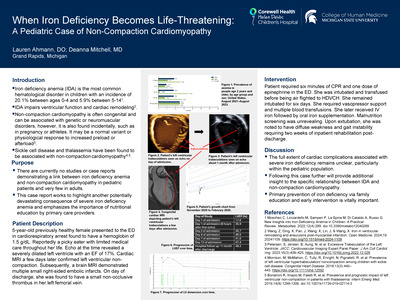
Viral Myocarditis in a 9-Month-Old Female: A Case Report
Madeline Deeb, Peter Wu, and Alysa Clark
Publication Date: 5-8-2026
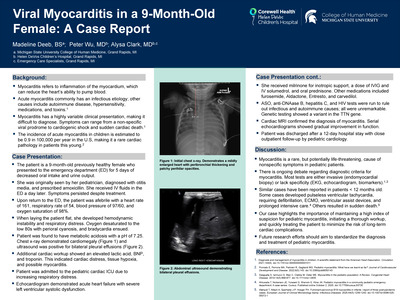
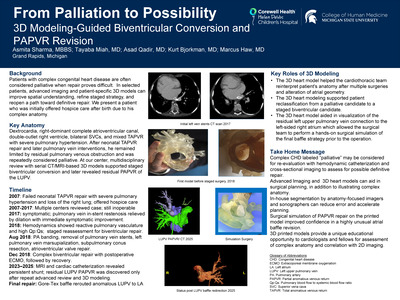
Myocarditis refers to inflammation of the myocardium, which can reduce the heart's ability to pump blood. Acute myocarditis commonly has an infectious etiology and the clinical presentation is highly variable; symptoms can range from a non-specific viral prodrome to cardiogenic shock and sudden cardiac death. The incidence rate of acute myocarditis in children is reported to be 0.9 in 100,000 per year in the U.S, making it a rare cardiac pathology in patients this young.
This case will discuss a 9-month-old previously healthy female who presented to the emergency department due to 5 days of poor oral intake and decreased urine output. She had originally been diagnosed with an ear infection by her primary care provider, but her symptoms persisted despite antibiotics. When the patient was laid flat on the exam table, she developed hemodynamic instability and respiratory distress. The patient's oxygen desaturated to the low 80s with bradycardia and perioral cyanosis. She was found to be in heart failure with bilateral pleural effusions and ascites, secondary to acute viral myocarditis.
This case highlights the importance of maintaining a high index of suspicion for pediatric myocarditis, initiating a thorough workup, and quickly treating the patient in order to minimize the risk of long-term cardiac complications. Although rare, myocarditis is a serious diagnosis that should always be kept on the differential for a pediatric patient with generalized refractory symptoms.
-

Synthetic Cannabinoid Use Complicated by Multiorgan Dysfunction
Jagroop Doad, Mckenna Galloway, and Jeremy Gentile
Publication Date: 5-8-2026
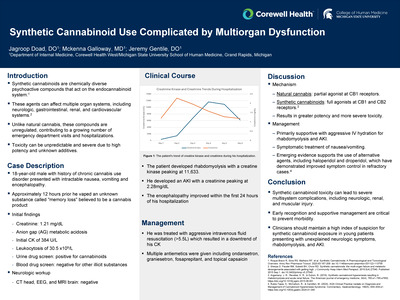
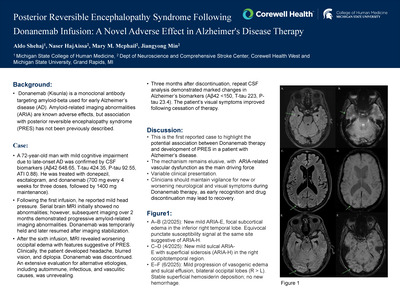
Synthetic cannabinoids are a chemically diverse group of psychoactive substances that target the endocannabinoid system and can cause severe, multisystem toxicity involving the neurologic, gastrointestinal, renal, and cardiovascular systems. Unlike natural cannabis, these compounds are unregulated, contributing to a growing number of emergency department visits and hospitalizations.� We present a case of synthetic cannabinoid use resulting in the constellation of seizures, encephalopathy, severe rhabdomyolysis, acute kidney injury (AKI), and refractory hyperemesis.
An 18-year-old man with a past medical history of chronic cannabis use disorder presented to the emergency department by EMS for acute confusion with intractable nausea and vomiting. Approximately 12 hours prior, he vaped an unknown substance obtained from a friend, described as "Memory Loss," believed to be a cannabis product. His father reported that the patient called him and seemed confused. During this call, the father heard periods of loud grunting and heavy breathing along with disorganized speech. On arrival, EMS found the patient in the bathroom, covered in vomit, confused, and disoriented. On arrival to the ED, the patient had no memory of these events, including how he arrived in the bathroom or calling and talking to his father. Initial labs showed creatinine 1.21 mg/dL and an anion gap of 27. Urine drug screens were positive for cannabinoids only.
This case illustrates the unpredictable multisystem toxicity associated with synthetic cannabinoid exposure, including neurologic injury, rhabdomyolysis, acute kidney injury, and hyperemesis. Given the increasing prevalence of these substances, clinicians should maintain a high index of suspicion for synthetic cannabinoids in patients presenting with unexplained toxicity. Early recognition and aggressive supportive management are essential to prevent morbidity, and awareness of emerging therapies for refractory cannabinoid hyperemesis may help improve outcomes.
-

A Rare Case of Catamenial Pneumothorax
Brit Eller, Jamie L Huizinga, Lindsay Snyder, and Inara Ismailova
Publication Date: 5-8-2026
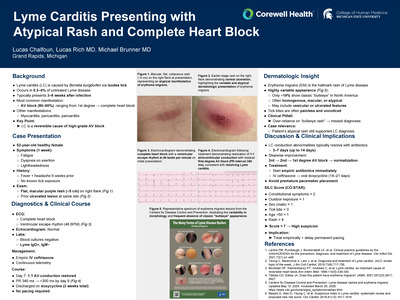
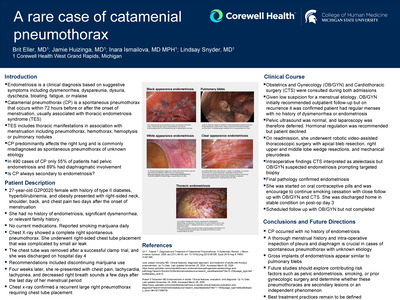
Catamenial pneumothorax is defined as spontaneous pneumothorax within 72 hours before or after the onset of menstruation and is usually associated with thoracic endometriosis syndrome (TES). Endometriosis is the presence of ectopic endometrial tissue outside the uterine cavity. TES includes thoracic manifestations in association with menstruation including pneumothorax, hemothorax, hemoptysis or pulmonary nodules. Catamenial pneumothorax predominantly affects the right lung and is commonly misdiagnosed as spontaneous pneumothorax of unknown etiology [1]. In a review of 490 cases of catamenial pneumothorax, only 55% of patients had pelvic endometriosis and 89% had diaphragmatic involvement [2]. This raises the question of whether catamenial pneumothorax is always secondary to endometriosis, particularly in patients without prior symptoms or diagnosis, as demonstrated in this case.
A 27-year-old G2P0020 female with a history of type II diabetes, hyperbilirubinemia, and obesity presented with right-sided neck, shoulder, back, and chest pain two days after the onset of menstruation. She had no history of endometriosis, significant dysmenorrhea, or relevant family history. She was not taking medications but reported smoking marijuana daily. Chest X-ray revealed a complete right spontaneous pneumothorax. She was hemodynamically stable and underwent right-sided chest tube placement. The air leak resolved by hospital day 3 without surgical intervention, allowing chest tube removal following a successful clamp trial. She was discharged on hospital day 4 with counseling to discontinue marijauna use. Four weeks later, she re-presented with chest pain, tachycardia, tachypnea, and decreased right breath sounds a few days after the last day of her menstrual period. Chest x-ray confirmed a recurrent large right pneumothorax requiring chest tube placement.
In this case, catamenial pneumothorax occurred without a history of endometriosis, highlighting the importance of a thorough menstrual history in cases of spontaneous pneumothorax with unknown etiology and intra-operative inspection of pleura and diaphragm. Future studies should explore contributing risk factors- pelvic endometriosis, smoking, or prior gynecologic surgery-and determine whether these pneumothoraces are true secondary lesions or an independent phenomenon. Best treatment practices remain to be defined.
-

Pulso Comunitario: A Community-Led Model for Trust-Centered Preventive Health Outreach
Tishanna Ferguson
Publication Date: 5-8-2026
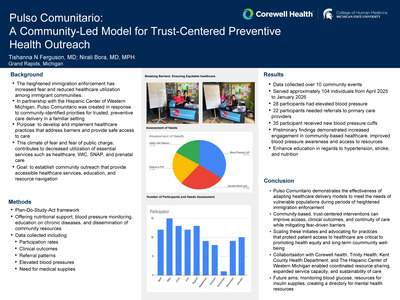
Recent immigration policy changes and the rescinding of the Department of Homeland Security's "sensitive areas" directive have heightened fear among vulnerable populations, including undocumented individuals, asylum seekers, and their families. This climate of fear has contributed to decreased utilization of essential services such as healthcare, WIC, SNAP, and prenatal care, leading to adverse health outcomes including malnutrition, worsening chronic disease, and increased fetal and infant morbidity and mortality. Pulso Comunitario was developed to address these barriers by creating trusted community hubs that provide accessible healthcare services, education, and resource navigation.
Methods: Using a Plan-Do-Study-Act (PDSA) quality improvement framework, community-based interventions were implemented in community centers to deliver low-barrier healthcare services. Offerings included nutrition support, blood pressure monitoring, education on chronic diseases, and dissemination of community resources. Data collected included participation rates, clinical outcomes, referral patterns, and health indicators such as elevated blood pressure and new diagnoses.
Across more than 10 community events, approximately 104 individuals were served. Twenty-two participants were referred to primary care for longitudinal follow-up, and 28 were identified with elevated blood pressure. Thirty-five individuals received home blood pressure cuffs to support ongoing monitoring. Preliminary findings demonstrated increased engagement in community-based healthcare, improved blood pressure awareness and control, identification of previously undiagnosed conditions, and enhanced medication adherence. Survey data revealed persistent fear of deportation as a barrier to traditional healthcare settings, while highlighting increased trust and utilization of community-based services. Additionally, reductions in emergency department utilization and complications from manageable chronic conditions were observed among participants.
Pulso Comunitario demonstrates the effectiveness of adapting healthcare delivery models to meet the needs of vulnerable populations during periods of heightened immigration enforcement. Community-based, trust-centered interventions can improve access, clinical outcomes, and continuity of care while mitigating fear-driven barriers. Scaling these initiatives and advocating for policies that protect patient access to healthcare are critical to promoting health equity and long-term community well-being.
-

From Terrarium to Tertiary Center: Managing a Mexican Beaded Lizard Hand Envenomation
Patrick Fewins, Keaboka Nyumbu, and Daniel Overbeek
Publication Date: 5-2026
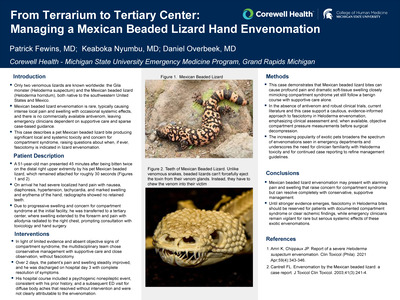
Only two venomous lizards are known worldwide: the Gila monster (Heloderma suspectum) and the Mexican beaded lizard (Heloderma horridum), both native to the southwestern United States and Mexico. Mexican beaded lizard envenomation is rare and typically produces intense local pain and swelling, with occasional systemic manifestations and no commercially available antivenom, leaving emergency clinicians reliant on supportive care and limited case-based guidance. This case describes a Mexican beaded lizard bite from a pet that produced significant local and systemic symptoms and raised concern for compartment syndrome, highlighting uncertainties regarding the role of fasciotomy in lizard envenomation.
A 51-year-old man presented 45 minutes after being bitten twice on the distal right upper extremity by his pet Mexican beaded lizard, which remained attached for approximately 30 seconds. On arrival, he reported severe localized pain and exhibited nausea, diaphoresis, hypertension, tachycardia, and marked swelling and erythema of the hand. Radiographs showed no retained teeth. Because of progressive swelling and concern for compartment syndrome at the initial facility, he was transferred to a tertiary center, where swelling extended to the forearm and pain with allodynia radiated to the right chest, prompting consultation with toxicology and hand surgery.
This case illustrates that Mexican beaded lizard envenomation can cause profound pain and dramatic soft-tissue swelling that may clinically resemble compartment syndrome yet still resolve with supportive management alone. In the absence of robust evidence or antivenom, current literature and this case support a cautious approach to fasciotomy in lizard bites, reserving surgical decompression for situations with objectively elevated compartment pressures or clear evidence of ischemia.
-

Coarctation of the Aorta Treated with TEVAR
Nicholas Fitzpatrick, Gruschen Veldtman, and Eanas Yassa
Publication Date: 5-8-2026
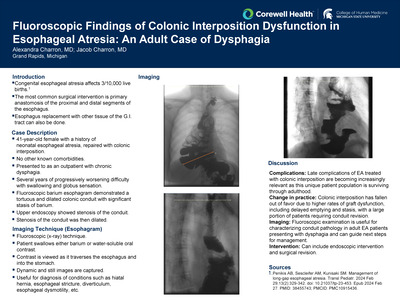
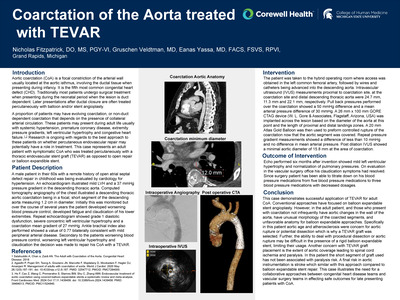
Aortic coarctation (CoA) is a focal constriction of the arterial wall usually located around the aortic isthmus and is the fifth most common congenital heart defect (CHD). Traditionally most patients undergo gold standard open repair during childhood but occasionally these lesions are missed or reoccur after repair with patients presenting in adulthood with symptoms of hypertension, claudication, extremity pressure gradients, left ventricular hypertrophy and congestive heart failure. Research is ongoing with regards to the best approach to these patients on whether percutaneous endovascular repair may potentially have a role in treatment. This case represents an adult patient with symptomatic aortic coarctation who was treated percutaneously with an endovascular stent graft as opposed to open repair or balloon expandible stent.
68-year-old male with a remote history of open atrial septal defect repair in childhood who was being evaluated by cardiology for hypertension was noted on echocardiogram to have mild LVH and mild PAH (RVSP 35 mmHg) and a 37-mmHg pressure gradient in the descending thoracic aorta. Computed tomography angiography of chest then illustrated a descending thoracic aortic coarctation measuring 1.2 cm in diameter. Initially this was monitored but over the course of several years the patient developed worsening blood pressure control, developed fatigue and claudication of his lower extremities. Repeat echocardiogram showed grade 1 diastolic dysfunction, severe concentric left ventricular hypertrophy and a coarctation mean gradient of 27- mmHg. Ankle brachial index was also performed showing a value of 0.77.
This case illustrates the changing paradigm in aortic coarctation treatment and how an endovascular approach with TEVAR in select patients who are optimal candidates over open surgical reconstruction is possible. The significant risk reduction associated with endovascular repair while also providing tangible clinical results shows the benefits of this approach in treatment. Greater collaborative efforts in this specific patient population at our institution will continue to provide more insight on which patients will benefit from TEVAR repair.
-
 Literature Search Tools in Medicine by Kimberly Forman, Rachel Armstrong, Allison Kowatch, Megan Courtley, Michelle Padley, Nawal Bennett, Tiffany Fleeger, Lindsey Ouellette, and Jeffrey Jones")
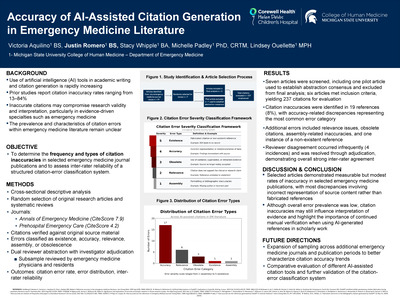
The Promise and Pitfalls of Artificial Intelligence (AI) Literature Search Tools in Medicine
Kimberly Forman, Rachel Armstrong, Allison Kowatch, Megan Courtley, Michelle Padley, Nawal Bennett, Tiffany Fleeger, Lindsey Ouellette, and Jeffrey Jones
Publication Date: 5-8-2026
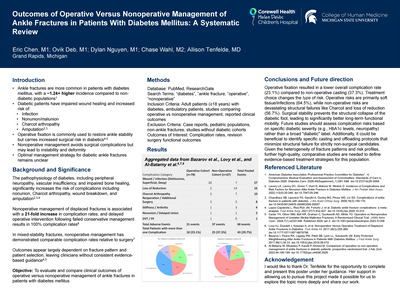
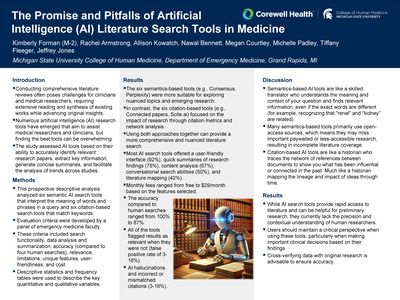
Conducting comprehensive literature reviews often poses challenges for clinicians and medical researchers, requiring extensive reading and synthesis of existing works while advancing original insights. Numerous artificial intelligence (AI) research tools have emerged to assist medical researchers and clinicians; however, identifying the most effective tools can be overwhelming. The study assessed AI tools for their ability to accurately identify relevant research papers, extract key information, generate concise summaries, and facilitate trend analysis across studies.
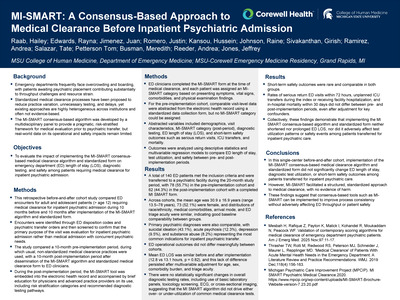
This prospective descriptive analysis examined six semantic AI search tools that interpret the meaning of words and phrases in a query, and six citation-based search tools that match keywords. A panel of emergency medicine faculty developed evaluation criteria. These criteria included search functionality, data analysis and summarization, accuracy (compared to four human searches), relevance, limitations, unique features, user-friendliness, and cost. Descriptive statistics and frequency tables were used to describe the key quantitative and qualitative variables.
The six semantics-based tools (e.g., Consensus, Perplexity) were more suitable for exploring nuanced topics and emerging research. In contrast, the six citation-based tools (e.g., Connected Papers, Scite.ai) focused on the impact of research through citation metrics and network analysis. Using both approaches together can provide a more comprehensive and nuanced literature search. Most AI search tools offered a user-friendly interface (92%), quick summaries of research findings (75%), content analysis (67%), conversational search abilities (50%), and literature mapping (42%). Monthly fees ranged from free to $29 per month/month based on the selected features. Accuracy relative to human searches ranged from 100% to 87%. All of the tools flagged results as relevant when they were not (false positive rate of 3-16%). AI hallucinations and incorrect or mismatched citations (3-16%).
AI-driven literature search tools have become increasingly sophisticated and accessible, providing substantial efficiencies in the identification and synthesis of medical evidence. Both semantic and citation-based systems offer unique advantages, and their combined use offers the greatest potential benefits for clinicians and researchers. Nevertheless, inherent risks-such as false positives and inaccurate citations-require users to maintain a critical, evaluative approach and avoid overreliance on automated outputs.
-

Ph+ T-cell ALL or CML Presenting in T-cell Blast Phase? A Case Report and Diagnostic Challenge
Caylee Forschner, Troy Quigg, and Allison Close
Publication Date: 5-8-2026
Philadelphia (Ph) chromosome, the defining feature of chronic myeloid leukemia (CML), is characterized by BCR:ABL1 gene translocation resulting in two oncogenic proteins, p190 and p210 (1). CML accounts for 3% of pediatric leukemias with 1-2% of cases presenting in blast phase (2, 3). The p210 fusion transcript is classically associated with chronic phase CML(1). The p190 transcript is commonly found in Ph+ acute lymphoblastic leukemia but is seen in 1-2% of CML(1). This can elicit diagnostic challenges in patients presenting with Ph+ T-cell ALL, an exceptionally rare diagnosis with only 30 cases reported in the literature(4). This report describe a case of Ph+ T-cell ALL with concern for CML in blast phase and highlight minimal residual disease (MRD) discordance between flow cytometry and BCR:ABL real time PCR (RT-PCR).
A 16-year-old male with 6 weeks of fatigue, URI symptoms and cervical lymphadenopathy, presented with massive splenomegaly, hyperleukocytosis (434K/uL), anemia (hgb 4.9 g/dL), thrombocytopenia (42 K/uL), and 97% peripheral blasts. Peripheral blood flow cytometry was consistent with T-ALL. FISH testing revealed BCR:ABL/t(9;22) gene fusion in 96.5% of nuclei and deletion of TCRB (7q34) region in 22% of cells. BCR:ABL RT-PCR demonstrated only a minor breakpoint (p190) fusion. He started treatment on AALL 1631 with imatinib for Ph+ T-cell ALL. Due to persistent disease at end of induction 1B with a MRD by flow cytometry of 2.3% and 8.5% by BCR:ABL RT-PCR, he transitioned to T-cell targeted treatment, NECTAR therapy with dasatinib. Following cycle 1 of this therapy, he had persistent MRD discordance, 0.072% by flow cytometry and 0.46% by BCR:ABL RT-PCR. Cell sorting demonstrated BCR:ABL positivity in both CD3 and CD15 cells, suggesting possible CML in T-cell blast phase.
Ph+ leukemias are uncommon in the pediatric population and association with T-ALL at any age is exceedingly rare. This case report highlights the diagnostic uncertainty in differentiating CML in blast phase from Ph+ T-ALL.
-

Impact of Ancillary Maneuvers in Deliveries with Increased Head to Body Delivery Intervals: A Retrospective Review
Hannah Garavaglia, Kate Wiewiora, and Lisa Thiel
Publication Date: 5-8-2026
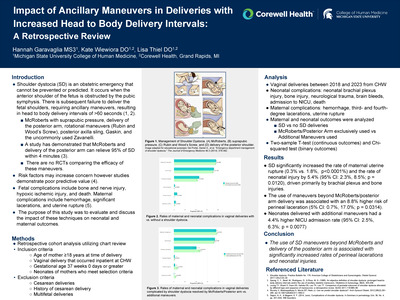
Shoulder dystocia (SD) is an obstetric emergency and is diagnosed during delivery when there is failure to deliver the fetal shoulders with gentle downward traction, resulting in the need for ancillary maneuvers and a head to body delivery interval (HBDI) of >60 seconds. Existing literature on the implications of ancillary maneuvers is limited, particularly those other than McRoberts maneuver and posterior arm delivery, given the poor predictive value of risk factors and the lack of randomized controlled trials comparing maneuvers for SD alleviation. The objective of this study is to evaluate the impact of additional maneuvers beyond McRoberts and posterior arm delivery on maternal and neonatal outcomes in vaginal deliveries complicated by shoulder dystocia.
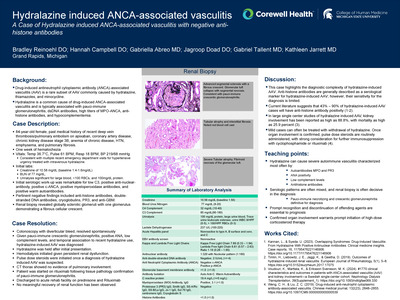
This retrospective cohort study evaluated 920 vaginal deliveries complicated by a shoulder dystocia with documented maneuvers from 2018 to 2023 to test the hypothesis that the use of ancillary maneuvers beyond McRoberts and posterior arm delivery is associated with higher maternal and fetal complication rates. Data from 178 shoulder dystocia-complicated deliveries only utilizing McRoberts and posterior arm maneuvers and 742 deliveries utilizing additional/other maneuvers were analyzed. Primary outcomes included maternal complications (hemorrhage, perineal lacerations, uterine rupture), neonatal complications (brachial plexus injury, bone injury, neurologic trauma, death), and NICU admission rates.
The use of maneuvers beyond McRoberts and posterior arm delivery was associated with an 8.8% higher risk of perineal laceration (95% CI: 0.7%, 17.0%; Chi-square p = 0.0314) and a 5.4% higher risk of newborn injury (95% CI: 2.3%, 8.5%; Chi-square p = 0.0120), driven primarily by brachial plexus and bone injuries. Neonates delivered with additional maneuvers also had a 4.4% higher NICU admission rate (95% CI: 2.5%, 6.3%; Chi-square p = 0.0077).
The use of delivery maneuvers beyond McRoberts and posterior arm delivery is associated with significantly increased rates of perineal lacerations and neonatal injuries. The rates of NICU admission are higher for neonates delivered with additional maneuvers, as expected given the clinical situations that require advanced maneuvers to resolve the shoulder dystocia. These results allow providers to properly counsel the women of our patient population who carry an elevated risks of shoulder dystocia during a vaginal delivery.
-

Rapid Whole Genome Sequence: A Level IV NICU Clinical Experience
Alexis George, Felicia White, Caleb Bupp, and Claudia Nadernejad
Publication Date: 5-8-2026
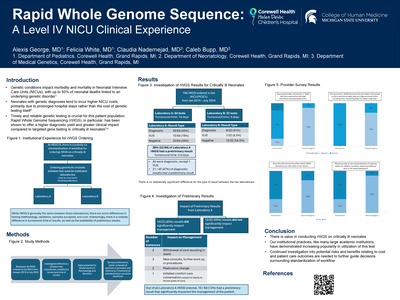
Genetic conditions impact morbidity and mortality in Neonatal Intensive Care Units (NICUs), with up to 50% of neonatal deaths linked to an underlying genetic disorder1. Additionally, neonates with genetic diagnoses tend to incur higher NICU costs, primarily due to prolonged hospital stays rather than the cost of genetic testing itself2. Therefore, timely and reliable genetic testing is crucial for this patient population. Rapid Whole Genome Sequencing (rWGS), in particular, has been shown to offer a higher diagnostic yield and greater clinical impact compared to targeted gene testing in critically ill neonates3,4. At HDVCH, there is currently no standardization of workflow for ordering rWGS in this patient population. The ordering geneticist chooses between two outside institution laboratories: "laboratory A" and "laboratory B" on a case-to-case basis as well as personal preference.
This study investigated our institutional experience of utilizing rWGS testing in our neonatal population and investigated differences between the two laboratories, notably the turnaround timing for results. The test characteristics of all rWGS ordered from January 2019 to July 2024 at our institution were reviewed. This data was presented to the providers within the Departments of Neonatology and Genetics, and a survey was conducted to collect general opinions of rWGS amongst these providers, as well as to determine if a standardization of workflow would be beneficial at our institution.
From January 2019 to July 2024, 106 rWGS were ordered on critically ill neonates; 84 of these were sent to "laboratory A" and 22 to "laboratory B." The turnaround time for rWGS results from "laboratory A" had a mean of 14 days, and 8 days for "laboratory B." There was no statistical significant difference for the type of result (diagnostic, variant of undetermined significance, negative) observed between the two laboratories. Interestingly, "laboratory A" offers preliminary results; 22 (26%) of rWGS sent to "laboratory A" had a preliminary result with a turnaround time of 3.8 days. All preliminary results carried a diagnostic result, except 1 variant of undetermined significance. Further investigation into the preliminary results demonstrated that 10 (45%) of the preliminary results did go on to significantly impact management of the patient. After presentation of this data to the providers within the Neonatology and Genetics Departments, surveys were conducted.
There is value in conducting rWGS on critically ill neonates and our institutional practices, like many large academic institutions, have demonstrated increasing popularity in utilization of this test. It is interesting to observe the disagreement between our Neonatology and Genetics departments regarding the perceived utility that a standardization of workflow regarding rWGS ordering habits within our institution would yield. Continued investigation into potential risks and benefits relating to cost and patient care outcomes are needed within to further guide decisions.
-

Diagnosis of Glycogen Storage Disease Type III in an Infant with Failure to Thrive
Jason Gilmore, Paige Juriga, and James Van Beynen
Publication Date: 5-8-2026
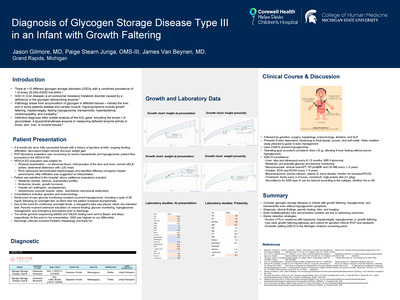
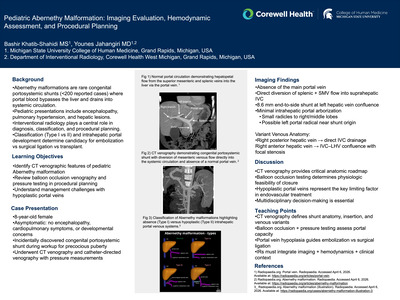
Glycogen storage disease type III (GSD III) is a rare inherited disorder of glycogen metabolism that can present in infancy with hypoglycemia, hepatomegaly, and growth failure. Early recognition is critical to prevent metabolic decompensation and long-term complications.
We present a 9-month-old, term, fully vaccinated female with a history of decreased height velocity and poor weight gain who was referred to the HDVCH emergency department after outpatient evaluation for failure to thrive revealed severe transaminitis (AST 1429 U/L, ALT 765 U/L) and hypoglycemia (blood glucose 39 mg/dL). On presentation, she was clinically well appearing. A broad diagnostic evaluation was initiated, including autoimmune, infectious, and metabolic studies. Right upper quadrant ultrasound demonstrated hepatomegaly with hepatic steatosis. Serial point-of-care glucose monitoring revealed recurrent hypoglycemia, including a nadir of 26 mg/dL following an overnight fast, at which time the patient remained asymptomatic. Critical laboratory evaluation showed hypertriglyceridemia, anion gap metabolic acidosis, elevated lactate dehydrogenase, neutropenia, and appropriately suppressed insulin and C-peptide levels. Echocardiogram showed no evidence of cardiomyopathy.
This case highlights the importance of considering glycogen storage diseases in infants presenting with failure to thrive, hypoglycemia, and transaminitis, even in the absence of symptoms during hypoglycemic episodes. Early multidisciplinary involvement and proactive nutritional management are essential to optimize outcomes.
-
 in Non-Invasive Emergency Department Reduction of an Inguinal Hernia by Antonio Gonzales and Jordan Johnson")
Use of Point of Care Ultrasound (POCUS) in Non-Invasive Emergency Department Reduction of an Inguinal Hernia
Antonio Gonzales and Jordan Johnson
Publication Date: 5-8-2026
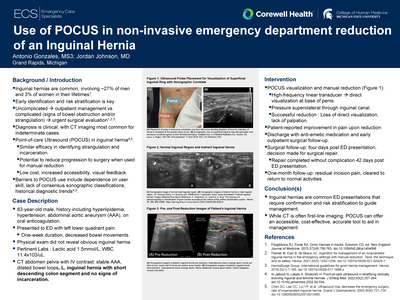
Inguinal hernias are common. Acute ED presentations require prompt diagnosis and risk stratification. Patients without signs of complication may undergo reduction and outpatient follow-up, whereas signs of bowel obstruction or strangulation necessitate urgent surgical evaluation. Diagnosis is often clinical, with adjunct imaging reserved for cases of uncertainty, most commonly computed tomography. Ultrasound demonstrates similar efficacy while offering advantages of low cost, accessibility, and rapid confirmation of reduction. Point-of-care ultrasound (POCUS) has shown comparable diagnostic accuracy, particularly in detecting incarceration and strangulation, and the potential to reduce progression to surgery when used during manual reduction of inguinal hernias. This case from a small, critical access ED highlights the utility of POCUS in managing hernia complications.
An 83-year-old male with past medical history including hypertension, hyperlipidemia, venous thromboembolism on anticoagulant medication, and abdominal aortic aneurysm (AAA) presented to a community-hospital emergency department for left lower quadrant (LLQ) abdominal pain and decreased bowel movements. The patient described one week of sharp, intermittent, 8/10 intensity pain with associated nausea and denied blood in his stool. Physical exam demonstrated LLQ abdominal tenderness, with no obvious hernia appreciated. The initial differential diagnosis included diverticulitis, bowel obstruction, and inguinal hernia. Pertinent lab values included Lactic acid 1.5 mmol/L, Bicarbonate 28 mmol/L, Creatinine 1.10 mg/dL and White Blood Cells 11.40 x103 /uL. A CT scan of the abdomen and pelvis with IV contrast was performed. Pertinent findings included a stable AAA, dilated loops of bowel, and a left inguinal hernia containing a short descending colon segment without signs of incarceration.
Inguinal hernias are a common emergency department presentation where prompt confirmation and risk stratification is required to guide management. Accurate distinction is critical, as complications such as bowel obstruction or strangulation require emergent surgical evaluation, whereas uncomplicated cases may be managed outpatient. While CT is often pursued, point of care ultrasound offers an accessible, cost-effective, accurate tool for physicians in the diagnosis, stratification of risk, and bedside management in patients presenting with inguinal hernias.
-

Discovery of a Sarcomatoid Malignancy in the Case of a Superior Mesenteric Vein and Portal Vein Thrombosis
Hamzah Hakkani, Tanya Hammoud, Clarice MacMillen, and James Morrison
Publication Date: 5-8-2026
Portal vein thrombosis (PVT) and superior mesenteric vein (SMV) thrombosis are uncommon but potentially life-threatening venous obstructions of the GI tract associated with cirrhosis,
A 56-year-old man without significant medical history presented with several months of intermittent abdominal pain. Upon further evaluation, CT imaging revealed extensive SMV thrombosis extending to the portal vein without evidence of bowel ischemia. Initial treatment included anticoagulation, however over subsequent weeks despite appropriate treatment and compliance with anticoagulation, the patient had worsening abdominal pain. Additional imaging at that time demonstrated propagation of thrombosis involving the right and main portal, splenic, and the superior and inferior mesenteric veins. Further work-up with hematology and oncology services during this time revealed no identifiable malignancy or hypercoagulable disorders. Given ongoing progression despite anticoagulation, interventional radiology services were consulted for consideration of thrombectomy.
This case illustrates the challenges of managing refractory venous thrombosis and as well as the limitations of repeated endovascular intervention in the absence of a clearly defined underlying etiology. Progressive thrombosis despite anticoagulation and technically successful IR therapy should prompt reassessment for occult malignancy as these may be early manifestations of aggressive malignancy.
-

Prolonged Inhaled Anesthetic Therapy for Refractory Status Asthmaticus
Reema Hamdan, Alec McKheen, and John Huntington
Publication Date: 5-8-2026
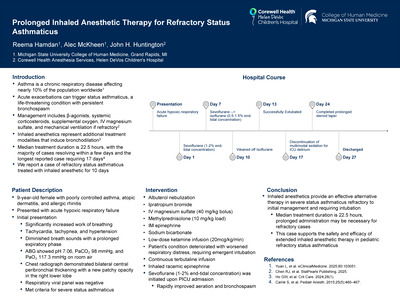
Asthma is a chronic respiratory disease affecting nearly 10% of the population worldwide. Acute exacerbations can trigger status asthmaticus, a life-threatening condition characterized by persistent bronchospasm unresponsive to standard medications, including bronchodilators and corticosteroids. Standard management includes high-dose inhaled β-agonists, systemic corticosteroids, supplemental oxygen, intravenous magnesium sulfate, and mechanical ventilation if refractory. However, some cases require further intervention. Inhaled anesthetics, especially sevoflurane and isoflurane, represent additional treatment modalities that induce bronchodilation. Median treatment duration is 22.5 hours, with the majority of cases resolving within a few days and the longest reported case requiring 17 days. We report a case of refractory status asthmaticus treated with inhaled anesthetic for 10 days.
A 9-year-old female with poorly controlled asthma, atopic dermatitis, and allergic rhinitis presented with acute hypoxic respiratory failure due to status asthmaticus. On initial presentation, physical exam revealed significantly increased work of breathing, tachycardia, tachypnea, hypertension, and diminished breath sounds with a prolonged expiratory phase. The patient was afebrile with SpO₂ 100% on room air. Initial arterial blood gas showed pH 7.06, PaCO₂ 98 mmHg, and PaO₂ 117.3 mmHg on room air. Chest radiograph demonstrated bilateral central peribronchial thickening with a new patchy opacity in the right lower lobe. Respiratory viral panel was negative. The patient met criteria for severe status asthmaticus based on persistent bronchospasm despite maximal medical therapy and impending respiratory failure.
In patients with severe status asthmaticus refractory to initial management requiring intubation, inhaled anesthetics provide an effective alternative therapy. While median treatment duration with inhaled anesthetics is 22.5 hours, prolonged administration may be necessary for refractory cases. This patient required 10 days of inhaled anesthetic treatment, representing one of the longer reported durations of use for status asthmaticus. This case supports the safety and efficacy of extended inhaled anesthetic therapy in pediatric refractory status asthmaticus.
-

Complete Atresia of the Vas Deferens: Routine Laparoscopic Hernia Repair as Catalyst in Diagnosis of Cystic Fibrosis
Tanya Hammoud, Matt Morris, Jessica Priestley, Carolyn Dress, and Elliot Pennington
Publication Date: 5-8-2026
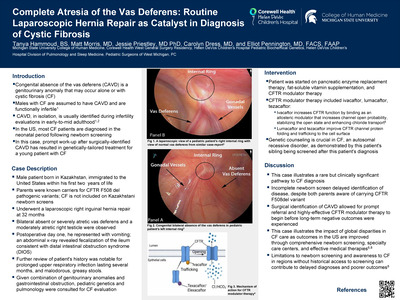
Congenital absence of the vas deferens (CAVD) is a well-established genitourinary manifestation that may occur alone or in association with cystic fibrosis (CF). As nearly all males with CF are assumed to have CAVD, in isolation, the condition is a spectrum of genitourinary malformations most commonly identified during infertility evaluations in early-to-mid adulthood. In the United States, the universal addition of CF to newborn screening programs has permitted pre-symptomatic diagnosis for the vast majority of patients. Here, we present a case for which this was not true. Instead, surgical identification of CAVD prompted work up for CF that facilitated genetically tailored treatment for a young patient with CF.
Our male patient was born in Kazakhstan to Russian parents and immigrated to the United States at 20 months of age. He was followed by a pediatric general surgeon for a communicating right hydrocele and underwent a laparoscopic right inguinal hernia repair at 32 months of age. Intraoperatively, bilateral absent or severely atretic vas deferens and a moderately atretic right testicle were identified, raising concern for CF. On postoperative day one, he returned with persistent vomiting and an abdominal x-ray revealed fecalization of the ileum consistent with distal intestinal obstruction syndrome (DIOS). He was admitted and treated with resolution of symptoms by the following day. Given the combination of genitourinary anomalies and gastrointestinal obstruction, pediatric pulmonology was consulted for cystic fibrosis evaluation.
Since 2010, the majority, but not all, U.S. CF diagnoses are precipitated by positive newborn screens. This case highlights a clinical manifestation of CF (CAVD), identified during hernia repair, hastening evaluation for the disease. Diagnosis enabled prompt initiation of tailored CF therapies, highlighting the importance of recognizing clinical CF manifestations in children. While success of screening and treatment in the developed world has allowed children with CF to reach adulthood, this same model of care has not been equitably applied across the developing world.
-

From Empiric to Intentional: Cryoprecipitate Utilization after Removal from a Massive Transfusion Order Set
Lexie Hampton, Justin Tran, Elizabeth Feuerstein, and Nada Naiyer
Publication Date: 5-8-2026
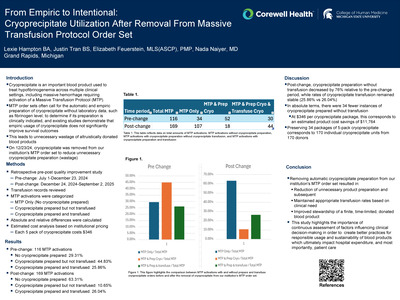
Cryoprecipitate is used to treat hypofibrinogenemia across multiple clinical settings, including massive hemorrhage, disseminated intravascular coagulation, and inherited fibrinogen disorders. Early and empiric transfusion of cryoprecipitate has not been shown to improve all-cause 28 day mortality, thus bringing into question the value of cryoprecipitate inclusion within a Massive Transfusion Protocol (MTP). Automatic cryoprecipitate preparation during MTP represents a source of avoidable waste, as the product is unlikely to be transfused to any individual and expires within 4 hours of thawing. On 12/23/24, cryoprecipitate was removed from our institution's MTP order set and transitioned to a provider-initiated manual order. This project's aim is decreasing cryoprecipitate wastage linked to MTP order sets by shifting to clinician‑directed ordering during MTP activations.
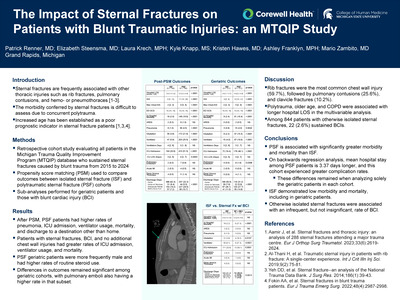
This study includes data from 07/01/2024 to 07/31/2025 with cryoprecipitate removal from the MTP order set on 12/25/2024, separating the data into pre-change and post-change period. MTPs and their associated cryoprecipitate orders, transfusions, and labs were reviewed. MTPs were categorized into three groups: no preparation or transfusion of cryoprecipitate; preparation of cryoprecipitate without transfusion; and both preparation and transfusion of cryoprecipitate. The absolute and relative differences of these three groups were compared before and after the change. Estimated cost impact was determined using institutional cryoprecipitate pricing.
Pre-change 116 MTP activations were identified. Of these, 29.31% had no cryoprecipitate use, 44.83% had cryoprecipitate preparation without transfusion, and 25.86% had both cryoprecipitate preparation and transfusion. Post-change 169 MTP activations were identified. Of these, 63.31% had no cryoprecipitate use, 10.65% had cryoprecipitate preparation without transfusion, and 26.04% had both cryoprecipitate preparation and transfusion. Post-change, cryoprecipitate preparation without transfusion decreased by 76% relative to the pre-change period, while rates of cryoprecipitate transfusion remained stable (25.86% vs 26.04%). In absolute terms, there were 34 fewer instances of cryoprecipitate prepared without transfusion, corresponding to a direct product cost savings of $11,764 at a cost of $346 per unit.
Removal of cryoprecipitate from the MTP order set was associated with a 76% reduction in unnecessary cryoprecipitate preparation while maintaining appropriate transfusion for patients who required it. This intervention improved blood product stewardship, decreased product wastage, and reduced direct product costs without limiting access when clinically indicated. These findings demonstrate that small protocol modifications can produce meaningful operational and stewardship gains in transfusion services.
-

Analysis of Optimal Excisional Margin for T2 Melanomas
Hyosung Han, Hannah Liefeld, and Gerald P. Wright
Publication Date: 5-8-2026
Melanoma is an aggressive form of skin cancer with a rising global incidence. Current National Comprehensive Cancer Network (NCCN) guidelines recommend surgical excision margins of 1-2cm for T2 melanomas (1-2 mm thickness) to balance local recurrence with quality of life. However, controversy persists regarding the optimal margin width within this range. While narrower margin may reduce surgical morbidity, cosmetic deformities, and healthcare costs, questions regarding their ability to maintain equivalent recurrence and survival outcomes remain unanswered. This study aims to evaluate recurrence rates, overall survival (OS) and disease-free survival (DFS) in a consecutive series of patients with T2 melanomas treated with 1cm versus 2cm surgical margins.
A retrospective analysis was conducted on patients diagnosed with T2 melanoma who underwent either 1cm or 2cm surgical excision margins at a single institution between 01/01/2014 to 01/01/2024. The primary outcome of interest was recurrence rate (local, nodal, or distant), with secondary outcome including OS, and DFS. Statistical comparisons were performed using unpaired t-tests or Mann-Whitney tests for quantitative variables, and Chi-square or Fisher's Exact tests for nominal variables, with statistical significance set at P< 0.05. Data were managed using a de-identified REDCap database. Results are pending.
-

Lumbar Sympathetic Ablation in the Treatment of Erythromelalgia: A Case Study and Review of Literature
Zoee Harris, Clarice MacMillen, and James Morrison
Publication Date: 5-8-2026
Erythromelalgia is a rare syndrome that presents with a classic triad of symptoms, including episodic redness, warmth, and burning pain in the extremities. It can be primary in nature or associated with thrombocytopenias or other medical conditions (secondary). Primary erythromelalgia is thought to be caused by changes in voltage-gated sodium channels on nociceptive receptors, leading to dysregulation of pain signals from nonpainful stimuli. Management of these patients can be difficult, as they are often resistant to treatment. Lumbar sympathetic ablation, a form of sympathectomy, is a potential treatment for erythromelalgia. However, only a handful of cases have been reported in the literature and long-term post-ablative outcomes are unknown. This exhibit outlines a case of successful lumbar sympathectomy in a patient with erythromelalgia that produced long lasting symptom improvement.
The patient is a 23 year old female, now diagnosed with erythromelalgia, who presented to the Corewell Health Grand Rapids Emergency Department for unrelenting foot and hand pain. She previously had an extensive outpatient workup for these symptoms, which was inconclusive. NSAIDs, colchicine, diclofenac gel, and gabapentin were trialed without relief. Inpatient evaluations from general medicine, infectious disease, neurology, and rheumatology revealed another grossly unremarkable workup. Popliteal nerve blocks were placed by anesthesia in preparation for a foot examination. These blocks completely resolved her symptoms, which recurred once the block wore off. Interventional Radiology was then consulted for a lumbar sympathetic nerve block, which was successful in reducing her symptoms. This was followed by a lumbar sympathetic nerve ablation given the nerve block success. The patient indicated 90% improvement in her pain symptoms for 17 months following the procedure.
This case demonstrates successful treatment of the debilitating symptoms of erythromelalgia using lumbar sympathetic ablation. Interestingly, the patient experienced improvement in both pain as well as the swelling and erythema in her lower extremities. With the procedure's minimally invasive nature and promising results, it has potential to be a preferred treatment option. More research is needed to integrate it into the management plan for erythromelalgia patients.
-

Cannabinoid Hyperemesis Versus Cyclic Vomiting Syndrome in Children Presenting to the Emergency Department
Jeffrey Haus, John Stathakios, Jennifer Hemberg, Peter van der Eb, Jessica Park, Nawal Bennett, Chen Shen, and Jeffrey Jones
Publication Date: 5-8-2026
Both cannabinoid hyperemesis syndrome (CHS) and cyclic vomiting syndrome (CVS) present with recurrent episodes of severe nausea, vomiting, and abdominal pain in the absence of identifiable organic pathology, leading to frequent misdiagnosis and unnecessary interventions. Despite overlapping clinical features, inconsistent literature makes differentiating between CHS and CVS challenging in children. This retrospective study aims to compare disease patterns, demographics, clinical features, and treatment outcomes between patients with CHS and CVS to develop a more pragmatic diagnostic approach.
This was a retrospective cohort analysis of consecutive children (< 18 years old) diagnosed with CHS or CVS. Patients were seen at eight emergency departments (EDs) over an 8-month study period. Spanning 13 counties in Michigan, affiliated institutions included five rural medical centers, two university-affiliated hospitals, and a children's tertiary care facility. Data collected included demographics, clinical features, and treatment outcomes in children with CHS versus CVS. The Kruskal-Wallis and unpaired t-tests were used to compare these two groups across key demographic and outcome variables.
During the study period, 111 children met the inclusion criteria, 36 (32.4%) had documented CHS, and 75 (67.6%) had CVS. Children with CHS were older (17.5 vs. 12.3 years; p < 0.001), predominantly male (57.1 vs. 42.7%; p = 0.157), and exhibited greater racial and ethnic diversity (p = 0.005). CHS patients presented with more abdominal pain (77.8 vs. 58.7%, p=0.049) and showed numerically higher rates of both depression (25.0 vs 12.0%, p = 0.083) and anxiety comorbidities (22.2% vs 9.3%, p = 0.064). Most patients with CVS (76.5%) had used cannabis within the past week. The CVS cohort was less likely to receive IV fluids (52.1% vs. 72.2%, p = 0.045), had a longer ED length of stay (10.9 vs. 6.0 hours, p = 0.053), and was more likely to be admitted (8.0% vs. 0%, p = 0.082).
Although CHS and CVS share similar symptomatology, this study identifies key demographic and clinical distinctions that may aid in early differentiation. CHS was more prevalent among older adolescents with recent cannabis use and greater racial diversity, whereas CVS occurred in younger children with longer emergency department stays and higher admission rates. These findings underscore the need for prospective studies to refine diagnostic criteria and optimize management strategies for pediatric patients with recurrent vomiting syndromes.
-

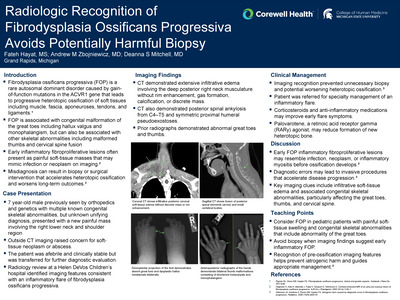
Radiologic Recognition of Fibrodysplasia Ossificans Progressiva Avoids Potentially Harmful Biopsy
Fateh Hayat, Andrew Zbojniewicz, and Deanna Mitchell
Publication Date: 5-8-2026
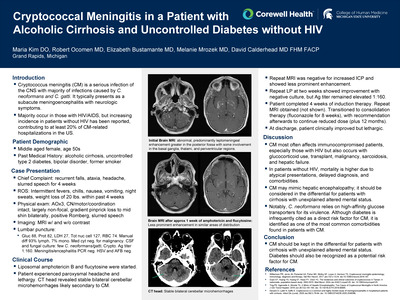
Fibrodysplasia ossificans progressiva (FOP) is a rare genetic disorder caused by gain of function mutations in the ACVR1 gene, leading to progressive heterotopic ossification of soft tissues. Early inflammatory flares can present as painful soft-tissue masses, which may mimic abscess or neoplasm on initial imaging. Misdiagnosis can result in unnecessary biopsies or surgery, which can exacerbate ossification. Prompt recognition of characteristic imaging findings can help prevent iatrogenic harm.
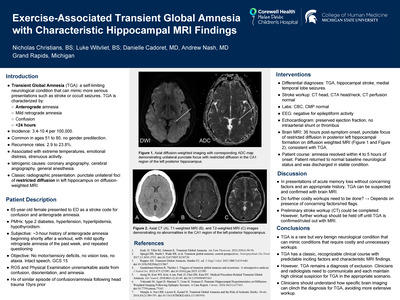
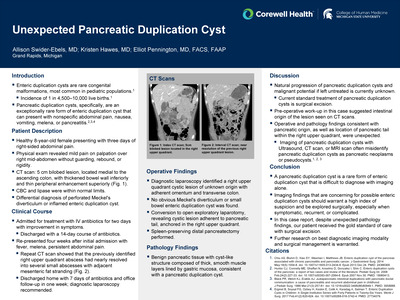
Patient Description: A 7-year-old boy with multiple congenital skeletal abnormalities presented with a new painful mass over the right lower neck and shoulder. He was initially seen at an outside urgent care and emergency department, where CT suggested possible soft-tissue neoplasm or abscess. He was afebrile and otherwise well. Due to diagnostic uncertainty and possible need for surgery, he was transferred to Helen DeVos Children's Hospital for further evaluation. Imaging Findings: Overread of the CT showed an extensive edematous, infiltrative process in the deep posterior neck muscles without discrete mass, rim enhancement, gas, or calcification. Additional findings included progressive posterior spinal ankylosis (C4-T5) and symmetric proximal humeral pseudoexostoses, consistent with chronic skeletal manifestations of FOP. Correlation with prior imaging and history supported an acute inflammatory flare rather than neoplasm or abscess.
This case underscores the important role of radiology in identifying FOP in acute pre-ossification flares, particularly because initial imaging can be concerning for infection or neoplasm. Early and accurate recognition can prevent unnecessary and potentially harmful interventions. Additionally, this case provides a valuable educational example of how careful integration of current imaging findings with prior imaging and clinical history can help guide management in rare skeletal disorders.
-

Navigating a Difficult Airway and Positioning Challenges in a Patient with Severe Ankylosing Spondylitis
Theodore Hoenke, Audrey Pham, and Caitlin Nemeth
Publication Date: 5-8-2026
Ankylosing spondylitis (AS) is a chronic, inflammatory autoimmune disease that involves structural spinal changes, which can pose increased risks for airway failure or spinal cord injury during intubation and airway management. AS may cause spinal ligaments to ossificate and the annulus fibrosis of the intervertebral disc(s) to calcify, resulting in a "bamboo spine" appearance on radiographic imaging. Physiological changes include a limited atlanto-occipital extension, restricted oral aperture, and positional intolerance while supine due to fixed cervical flexion from spinal fusion. As such, airway management and positioning for patients with AS requires a careful, individualized approach.
A 75 year old male with AS, essential HTN, and GERD presented to the ED after a fall carrying his groceries. On exam, he showed decreased BLE sensation, 0/5 strength in his lower extremities, and exaggerated cervical kyphosis. CT of his cervical spine demonstrated a nondisplaced transverse fracture through the mid body of T1, a nondisplaced fracture of the posterior lamina of C7 bilaterally, and an epidural hematoma at C6-T2. MRI was considered but due to significant kyphosis, there was a concern that he could not fit in the machine. Due to his progressing complete paraplegia, it was decided that an emergent laminectomy and evacuation of the spinal hematoma needed to be done.
Careful preoperative planning and communication between healthcare teams is essential for safe positioning and intubation for AS patients with severe kyphosis. Videolaryngoscopy must be avoided due to the risk of a hyperextension injury to the neck. Awake nasal fiberoptic intubation with topical anesthesia is the gold standard for AS patients with severe cervical kyphosis. When placing such patients in the prone position rigid head stabilization and proper padding are needed to maintain spinal curvature and prevent iatrogenic injury.
-

Efficacy and Safety of a Nurse-Driven Heparin Protocol During Atrial Fibrillation Ablation
Matthew Hollowell, Jack Tietema, Jagienka Timek, Joseph Banno, Anastasia Bury, Theresa Pasion, Andre J. Gauri, Sanjay Dandamudi, and Nagib Chalfoun
Publication Date: 5-8-2026
Atrial fibrillation (AF) is a common arrhythmia with significant morbidity and mortality, affecting at least 10.5 million people in the U.S. alone . Though pharmacological therapy exists to mitigate symptoms and progression of AF, ablation procedures are considered the mainstay and often definitive treatment for AF . Despite its safety and efficacy, the procedure involves risk of thromboembolic events, namely stroke, fatal bleeding, and cardiac tamponade. Administration of anticoagulants, specifically heparin, during AF ablation is critical to minimize complications. However, there is a lack of consensus regarding how to achieve therapeutic activating clotting times (ACT) amongst published protocols. The objective of the present study is to assess the efficacy and safety of a nurse-driven, ACT-guided heparin protocol in patients undergoing AF ablation.
In this retrospective study from 7/1/2022 and 4/30/2023, patients undergoing AF ablation received weight-adjusted, nurse-administered heparin management targeting an ACT ≥ 350 seconds. Efficacy endpoints included time to target ACT and percentage of ACT values within the therapeutic range. Safety was assessed by the incidence of 30-day stroke, bleeding events, and mortality. The data was then compared across different BMI categories (< 25 kg/m2, 25-30 kg/m2, BMI >30 kg/m2) to assess consistency in outcomes and identify potential variations in efficacy and safety.
Of the 476 patients who underwent AF ablation, 336 achieved a therapeutic ACT following an initial heparin loading dose, with a mean time of 18 minutes to reach the target. Thirty-day stroke incidence was low (0.4%), and major bleeding occurred in 0.2% of patients. Minor bleeding events and rehospitalizations were observed in 3.3% and 4.8% of patients respectively.
The nurse-driven, ACT-guided heparin protocol efficiently and safely achieved therapeutic ACT values with minimal adverse effects. Moreover, the success of our protocol and achievement of therapeutic ACT values did not necessitate adjustments to preexisting DOAC use. These findings support an objective, streamlined, and standardized approach to anticoagulation during AF ablation with minimal physician guidance.
-

The Role of Creatine Supplementation in Post-Stroke Rehabilitation: Promising but Still Unresolved
Minahil Iqbal, Mariam Akmal, Esam Abobaker, Shayan Marsia, and Jiangyong Min
Publication Date: 5-8-2026
Stroke is a major cause of long-term disability, often leading to functional impairment. Beyond neurological damage, stroke-related sarcopenia from immobility and inflammation worsens recovery outcomes. Creatine, which enhances energy metabolism and shows neuroprotective properties, has been proposed as an adjunct therapy to improve functional rehabilitation after stroke. This systematic review evaluates the safety, efficacy, and potential mechanisms of creatine supplementation in stroke recovery.
MEDLINE, Embase, and CENTRAL databases were systematically searched till October 1, 2025 assessing creatine use in stroke survivors. Eligible designs were randomized or interventional studies assessing muscle mass, strength, mobility, and inflammatory outcomes of creatine supplement for post stroke recovery. Data was extracted and appraised using standardized quality assessment tools, and findings were narratively synthesized due to heterogeneity among studies.
Three studies (n=71) were included from 1,167 studies screened, with a mean follow-up duration of 58 days. Across three studies, creatine supplementation in stroke showed mixed results. The ICaRUS Trial (10 g/day for 7 days) found no improvement in muscle or functional recovery but noted reduced serum progranulin, suggesting anti-inflammatory effects. Butchart et al. reported better walking performance with creatine plus resistance training, while Meulengracht et al. found no functional or endurance benefits with creatine and maltodextrin. Overall, creatine was safe, well tolerated, and showed no adverse effects.
Creatine appears safe and may improve functional recovery, particularly with exercise in post-stroke patients. Limited evidence, by small sample sizes and methodological variability, suggests potential anti-inflammatory and neuroplastic effects. Larger, high-quality randomized controlled trials are needed to define optimal dosing, timing, and therapeutic efficacy in mitigating stroke-related sarcopenia and enhancing recovery outcomes.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.