


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
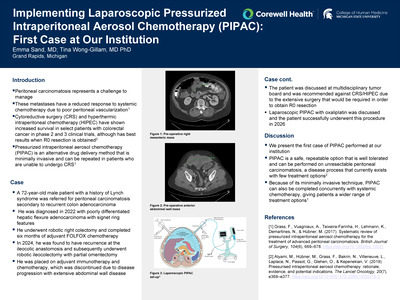
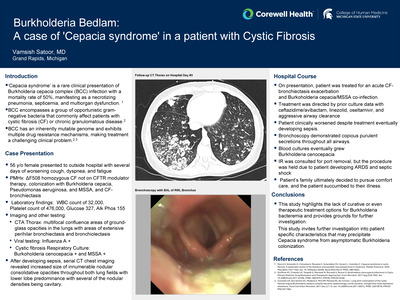
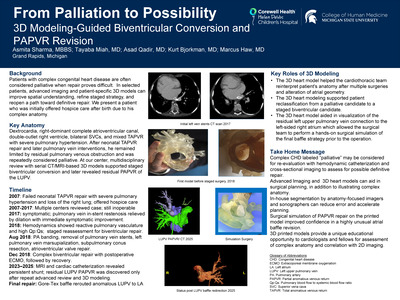
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-

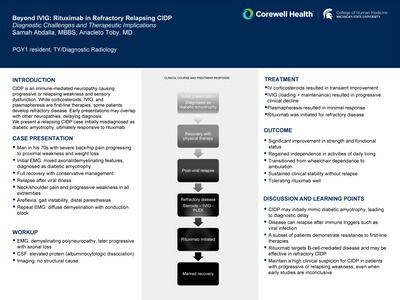
Warburg Effect in a 63-Year-Old T-Cell Lymphoma Patient with Pneumoperitoneum
Logan Jurgens and Nicholas Watson
Publication Date: 5-8-2026
The Warburg effect, first described in the 1920s by Otto Warburg, refers to "aerobic glycolysis"-a phenomenon in which malignant cells preferentially produce large amounts of lactate despite adequate oxygen availability. This effect is a recognized cause of type B lactic acidosis, which is defined as elevated serum lactate occurring in the absence of tissue hypoxia, unlike type A lactic acidosis, which is typically due to hypoperfusion or shock. Type B lactic acidosis is most associated with underlying conditions such as malignancy, liver disease, or certain medications. The Warburg effect is particularly seen in hematologic malignancies such as leukemia and lymphoma. In critically ill patients, where elevated lactate levels are often attributed to sepsis or ischemia, recognizing type B lactic acidosis due to the Warburg effect can be especially challenging, potentially delaying diagnosis.
A 63-year-old male with a recent diagnosis of T-cell lymphoma presented with pneumoperitoneum identified by CT imaging at an outside hospital. He underwent a small bowel resection with primary anastomosis and placement of a Jackson-Pratt drain. On admission, his lactate level was 1.8 mmol/L. However, by hospital day 8, he developed worsening tachycardia and hypotension. A repeat CT scan revealed a growing intra-abdominal hematoma, and his lactate had risen to 10.3 mmol/L. The hematoma was treated with interventional radiology-guided embolization. Despite intravenous crystalloid resuscitation, there was only mild improvement in lactate levels. Importantly, there was no evidence of respiratory failure, ongoing sepsis, or bowel ischemia. Nevertheless, lactic acidosis persisted even as the pneumoperitoneum and hematoma began to resolve. By hospital day 11, his lactate had further increased to 11.3 mmol/L, without any clinical or radiographic signs of infection or ischemia.
The patient presented with a complex clinical picture, including pneumoperitoneum, sepsis, and poor nutritional intake, which necessitated further evaluation. In critically ill patients, elevated lactate levels in the absence of hypoxemia, shock, ischemia, or liver dysfunction should raise suspicion for type B lactic acidosis. Importantly, lactic acidosis due to the Warburg effect is often resistant to conventional treatments such as IV fluids, corticosteroids, and thiamine. Warburg effect should be considered in lymphoma patients with no clear etiology.
-

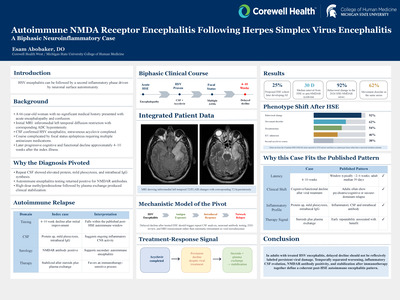
Understanding the Appeal and Amplification of Hazardous TikTok Challenges: A Thematic Analysis
Aleezay Khan, Abby Shah, Alex Schafer, Abriel Reister, Emma Lindemann, Brian Lewis, Andrea Reeder, Maddie Poll, and Jeffrey Jones
Publication Date: 5-8-2026
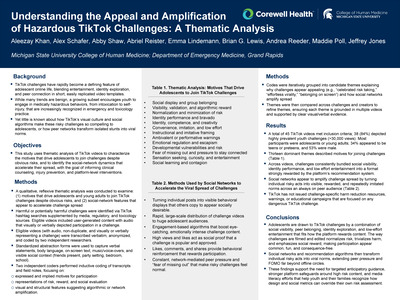
TikTok challenges are a prominent feature of adolescent online life, and a growing subset promote medically hazardous behaviors (for example, intoxication, self‑injury) increasingly encountered in emergency and toxicology practice. How TikTok's visual culture, social networks, and algorithms make these risky challenges appealing and viral among youth remains poorly characterized. Our objective was to (1) identify motives that drive adolescents and young adults to participate in hazardous TikTok challenges despite obvious risks, and (2) describe social‑network mechanisms that appear to accelerate the spread of these challenges.
A qualitative, reflexive thematic analysis of TikTok videos depicting harmful or potentially harmful challenges was conducted. Videos were identified via TikTok hashtag searches supplemented by media, regulatory, and toxicology sources; eligible user‑generated videos visually or verbally depicted challenge participation and contained audio. Transcripts and field notes captured spoken content, on‑screen text, music/voice‑overs, visible social context, and basic engagement indicators. Two independent coders performed inductive coding focused on expressed/implied motives, portrayals of risk and reward, and visual/structural markers of algorithmic or network amplification; codes were iteratively organized into themes supported by multiple videos.
Forty-five videos met the inclusion criteria; 38 (84%) depicted highly prevalent youth challenges (>30,000 views). Most participants appeared to be adolescents or young adults; 34% were identifiable as teens or preteens, and 53% as male. Thirteen themes were described that motivated participation, including social display and group belonging, visibility and algorithmic reward, and the normalization/minimization of risk. Network-level themes indicated that social platforms amplified the spread by transforming individual risky acts into visible, repeatedly imitated norms through high-speed distribution, engagement-based ranking, social proof (views/likes), and continuous, network-mediated peer pressure. No challenge-specific harm reduction warnings or education from TikTok were observed.
Hazardous TikTok challenges appear compelling to adolescents because they tightly couple developmental motives (belonging, identity exploration, sensation seeking, FOMO) with algorithmically rewarded visibility and peer approval. Findings support the need for anticipatory guidance in clinical encounters, stronger platform‑level safeguards around high‑risk challenge content, and media‑literacy efforts that help youth and families recognize how design and social metrics can override individual risk assessment.
-

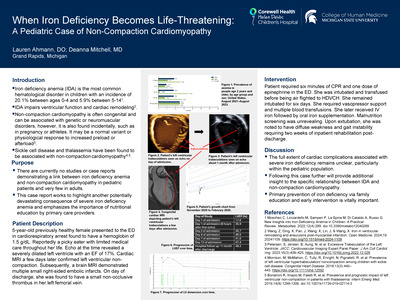
Histoplasmosis-Induced Hemophagocytic Lymphohistiocytosis in an Adult Patient on Immunosuppressive Therapy
Aryaan Khan, Syed Zawwar Zia, and Zachary Yono
Publication Date: 5-8-2026
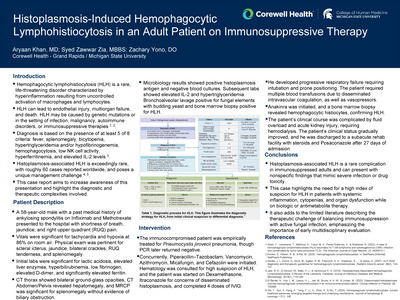
Hemophagocytic lymphohistiocytosis (HLH) is a rare, life-threatening disorder characterized by hyperinflammation resulting from uncontrolled activation of macrophages and lymphocytes. HLH can lead to endothelial injury, multiorgan failure, and death. HLH may be caused by genetic mutations or in the setting of infection, malignancy, autoimmune disorders, or immunosuppressive therapies 1, 2. Diagnosis is based on the presence of at least 5 of 8 criteria: fever, splenomegaly, bicytopenia, hypertriglyceridemia and/or hypofibrinogenemia, hemophagocytosis, low NK cell activity, hyperferritinemia, and elevated IL-2 levels 3. Histoplasmosis-associated HLH is exceedingly rare, with roughly 60 cases reported worldwide, and poses a unique management challenge 4, 5. This case report aims to increase awareness of this presentation and highlight the diagnostic and therapeutic complexities involved.
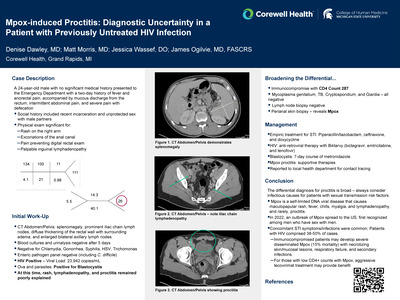
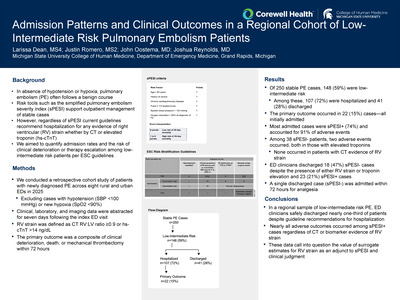
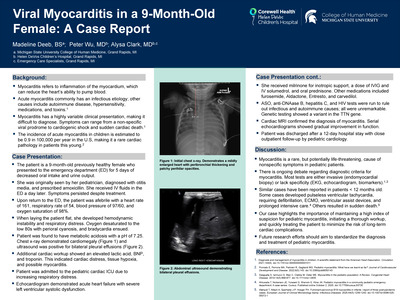
A 58-year-old male with a past medical history of ankylosing spondylitis on Infliximab and Methotrexate presented to the hospital with shortness of breath, jaundice, and right upper quadrant (RUQ) pain. Vitals were significant for tachycardia and hypoxia at 86% on room air. Physical exam was pertinent for scleral icterus, jaundice, bilateral crackles, RUQ tenderness, and splenomegaly. Initial labs were significant for lactic acidosis, elevated liver enzymes, hyperbilirubinemia, low fibrinogen, elevated D-dimer, and significantly elevated ferritin. CT thorax showed bilateral ground-glass opacities, CT Abdomen/Pelvis revealed hepatomegaly, and MRCP was significant for splenomegaly without evidence of biliary obstruction. Microbiology results showed positive histoplasmosis antigen and negative blood cultures. Subsequent labs showed elevated IL-2 and hypertriglyceridemia. Bronchoalveolar lavage positive for fungal elements with budding yeast and bone marrow biopsy positive for HLH.
Histoplasmosis-associated HLH is a rare complication in immunosuppressed adults and can present with nonspecific findings that mimic severe infection or drug toxicity. This case highlights the need for a high index of suspicion for HLH in patients with systemic inflammation, cytopenias, and organ dysfunction while on biologic or antimetabolite therapy. It also adds to the limited literature describing the therapeutic challenge of balancing immunosuppression with active fungal infection, emphasizing the importance of early multidisciplinary evaluation.
-

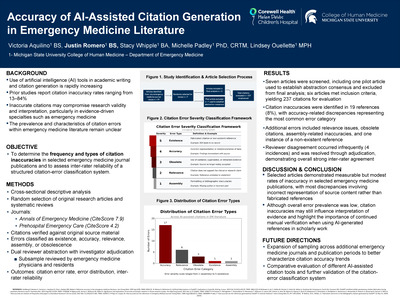
Pediatric Abernethy Malformation: Imaging Evaluation, Hemodynamic Assessment, and Procedural Planning
Bashir Khatib-Shahidi
Publication Date: 5-8-2026
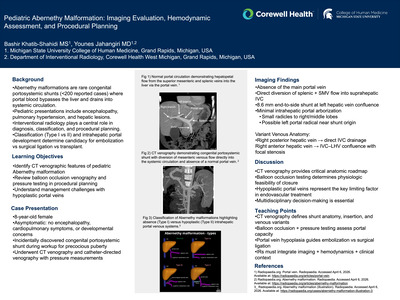
Abernethy malformations are rare congenital portosystemic shunts (< 200 reported cases) where portal blood bypasses the liver and drains into systemic circulation. Pediatric patients may present with encephalopathy, pulmonary hypertension, or hepatic lesions. Interventional radiologists are central to diagnosis and management. Accurate classification (Type I vs II) and evaluation of intrahepatic portal arborization are essential to determine candidacy for endovascular closure versus surgical ligation or transplant.
An 8-year-old girl was evaluated after an abdominal ultrasound (US) revealed multiple hepatic nodules up to ~4 cm in size and an anomalous connection between the portal vein and IVC. She was clinically well without neurological symptoms or signs of encephalopathy. However, laboratory tests showed mild liver dysfunction and shunt-related metabolic abnormalities. Her serum bilirubin and liver enzymes were mildly elevated, and blood ammonia was ~80 µmol/L (normal < 50). Notably, her prothrombin time was prolonged, reflecting reduced synthetic liver function, though no coagulopathy-related symptoms were present. Given the combination of large hepatic lesions and hyperammonemia in a child with a portosystemic shunt, a comprehensive workup was undertaken to characterize the nodules and plan for definitive treatment.
1) CT venography defines precise Abernathy malformation anatomy (shunt caliber, insertion site, venous anomalies) 2) Balloon occlusion and pressure testing assesses portal capacity and tolerance for shunt closure 3) Distinguishing hypoplastic from absent intrahepatic portal veins is key to selecting transcatheter vs surgical management 4) IRs must integrate imaging, hemodynamics, and multidisciplinary input when planning interventions.
-

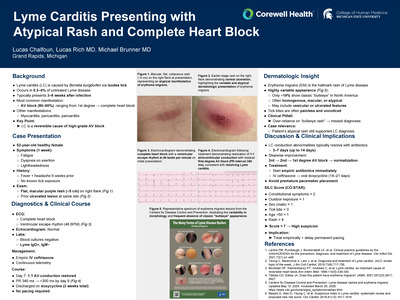
A Case of Cryptococcal Meningitis in a Patient with Alcoholic Cirrhosis and Uncontrolled Diabetes without HIV
Maria Kim, Robert Ocomen, Elizabeth Jakubowski Bustamante, Melanie Mrozek, and David Calderhead
Publication Date: 5-8-2026
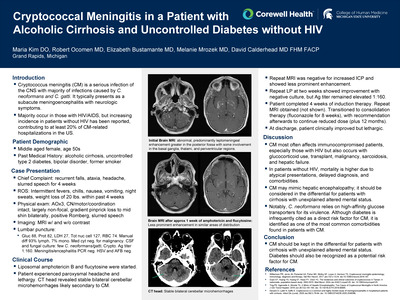
Cryptococcus meningitis (CM) is a serious infection of the CNS with the majority of infections caused by C. neoformans and C. gatti. It typically presents as a subacute meningoencephalitis with neurologic symptoms. Majority occur in those with HIV/AIDS, but increasing incidence in non-HIV patients has been reported, contributing to at least 20% of CM-related hospitalizations in the US.
A 55-year-old female with alcoholic cirrhosis, uncontrolled type 2 diabetes, bipolar disorder, former smoker presented with four weeks of recurrent falls, ataxia, and slurred speech, along with fever, chills, and headache. Labs were significant for Na 131, glucose 323, ALP 185, mild transaminitis, PLT 83, HA1c 8.3. Remainder of CBC, CMP, BHB, ammonia, ceruloplasmin, HIV, syphilis, hepatitis panel, drug screen, nutritional and infectious workup were unremarkable. Brain MRI showed abnormal, predominantly leptomeningeal, enhancement greater in the posterior fossa with some involvement in the basal ganglia, thalami, and periventricular regions. Neurology performed LP that showed elevated protein with lymphocytic pleocytosis, cryptococcus antigen 1:160 titer, and positive culture for cryptococcus neoformans/gatti. Blood cryptococcus antigen was negative.
CM most often affects immunocompromised patients, especially those with HIV, but also occurs with glucocorticoid use, transplant, malignancy, sarcoidosis, and hepatic failure. In non-HIV patients, mortality is higher due to atypical presentations, delayed diagnosis, and comorbidities. CM should be kept in the differential for patients with cirrhosis with unexplained altered mental status, as it may mimic hepatic encephalopathy. C. neoformans relies on high-affinity glucose transporters for virulence; uncontrolled diabetes should also be seen as a risk factor for CM.
-

Hepatitis C Screening and Treatment Pre and Post-Implementation of the USPSTF Universal Screening Guideline in Corewell Health Family Medicine Residency Clinics
Nolan Klunder, Harland Holman, and Nicholas Andersen
Publication Date: 5-8-2026
In March of 2020, the USPSTF updated guidelines to recommend a one-time screening for Hepatitis C for all patients regardless of risk. With this in mind, the World Health Organization (WHO) has established a goal of 90% of eligible patients being screened for Hepatitis C by 2030. It is not known how close to this goal Corewell Health is, nor how this implementation of universal screening has impacted identification and treatment of hepatitis C, including the proportion of patients treated by PCP vs a medical specialist.
A retrospective chart review of patients with at least one visit to the Corewell Health West Family Medicine Residency clinics between November 1, 2017 to December 31, 2025. Of this total population, the proportion of those who received a hepatitis C screening was measured to compare to The Who's 90% goal. Additionally, the number of patients who received treatment was measured and whether it was received by PCP or by a specialist. Furthermore, rates are compared between years to identify how and when the changes in practice recommendations have impacted identification and treatment of hepatitis C.
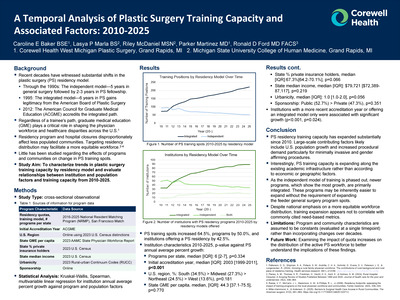
Data are still being gathered, however preliminary data shows that of the population of Family Medicine Residency clinic patients (Greenville and Grand Rapids locations), 103 patients had positive Hepatitis C antibodies between 2017 and 2023, of those 103 positive antibody tests, 38 were RNA positive, with 27 receiving treatment (20 by a Specialist vs. 7 by their PCP). After March of 2020, 11 patients were found to have positive antibody screenings, with 7 receiving treatment (4 by Specialists and 3 by PCP). Therefore, this limited data showed a large treatment gap (7 of 11 identified cases receiving treatment).
The implementation of universal screening for Hepatitis C has not only resulted in higher screening rates and identification of more cases of Hepatitis C, but also has empowered treatment in the Primary Care Setting and therefore removed barriers to treatment and resulted in higher levels of treatment and cure.
-

Geographic Access to MRI Machines and the Role of Mobile Imaging Units Across Michigan Counties
Connor Latterman and Joseph Junewick
Publication Date: 5-8-2026
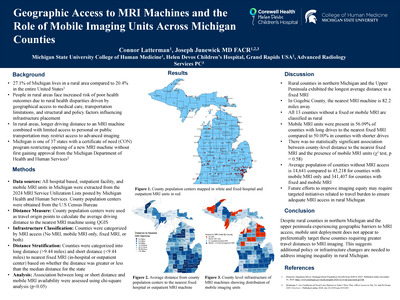
Rural populations face higher risks of poor health outcomes in part due to limited access to diagnostic imaging. Geographical barriers may be exacerbated by longer travel distances, limited public transportation, and structural and policy factors such as Certificate of Need (CON) regulations. Mobile MRI units have been deployed across Michigan; however, it remains unclear whether they are deployed in a manner that meaningfully reduces geographic barriers to MRI access in rural populations. This study examines geographic disparities in access to MRI machines across Michigan counties and evaluates whether current mobile MRI unit deployment aligns with counties experiencing the greatest travel burden.
All hospital based, outpatient facility, and mobile MRI units were extracted from the 2024 MRI Service Utilization Lists posted by Michigan Health and Human Services. County population centers were retrieved from the U.S Census Bureau and used as travel origins to determine the distance to the nearest fixed MRI unit in each county using QGIS. Each county was characterized by MRI access (No MRI, mobile MRI only, fixed MRI, or both) and categorized into long (>9.44 miles) and short distance (< 9.44 miles) to the nearest fixed MRI based on whether the distance was greater or less than the median distance for the state. Association between long and short distance and mobile MRI availability were assessed using chi-square analysis (p< 0.05).
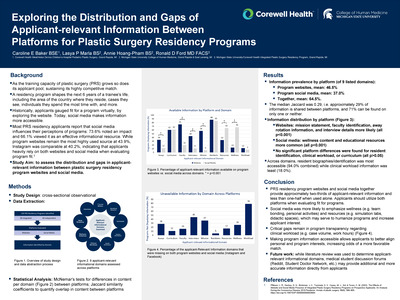
Rural counties in northern Michigan and the Upper Peninsula exhibited the longest average driving distance to a fixed MRI. Mobile MRI units were present in 56.09% of counties with long drives to the nearest fixed MRI versus 50.00% in counties with shorter drives. There was no statistically significant association between county-level distance to the nearest fixed MRI and the presence of mobile MRI units (chi-square test, p=0.58). Counties without MRI access had markedly smaller average populations (14,641) compared with counties served by mobile MRI only (45,218).
Despite rural counties in northern Michigan and the upper peninsula experiencing geographic barriers to MRI access, mobile unit deployment does not appear to preferentially target these counties requiring greater travel distances to MRI imaging. These findings highlight a potential mismatch between geographic need and mobile MRI deployment, highlighting the need for data-driven strategies to improve imaging equity in rural communities.
-
Special Considerations for Treating Pain in a Patient with Metastatic Cancer and Cocaine Use Disorder: A Case Report
Erin Leach
Publication Date: 5-8-2026
Patients with substance use disorders who are subjected to abrupt discontinuation of opioids for chronic cancer related pain are at increased risk for withdrawal, overdose, suicide, and hospital visits. Palliative care focused on harm reduction and patient retention strategies can lead to more optimal outcomes for these patients.
The patient is a 67-year-old female with a history of metastatic cholangiocarcinoma undergoing chemotherapy, chronic lumbar back pain, chronic hepatitis C, and substance use disorder in remission. She was referred to palliative care who assumed cancer pain management. While under their care, she tested positive for cocaine on a urine drug screen resulting in her opioids being abruptly deprescribed over safety concerns. Uncontrolled pain led to increased cocaine use, frequent ED visits, and recurrent hospitalizations for pain crises and risk of nosocomial infections.
Despite the need for palliative care in this unique patient population, the perceived risk of prescribing opioids is often viewed as too high by providers. As evidenced by this patient, pain management focused on harm reduction and patient retention philosophy may mitigate those risks. This presentation reviews clinical and social challenges in delivering palliative care to a cancer patient with active substance use disorder, and identify areas of future research, including methods of safe monitoring for high-risk patients requiring opioids for cancer-related pain.
-

Spring Assisted Cranioplasty versus Strip Craniectomy for Metopic Synostosis: A Comparison of Treatment Timelines and Craniometrics in the First Postoperative Year
Rachel Lee, Caroline Baker, Samuel Girian, Sarah Rushing, Brook Dudick, John Girotto, and Anna Carlson
Publication Date: 5-8-2026
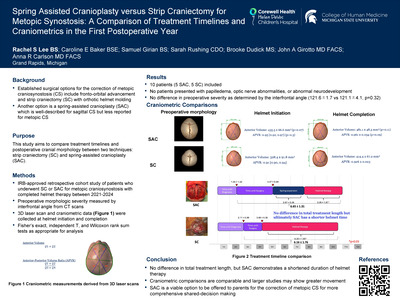
Strip craniectomy (SC) is a well-established for the correction of metopic craniosynostosis that relies on postoperative orthotic helmet molding to guide cranial reshaping over time. Spring-assisted cranioplasty (SAC) is a less frequently described treatment that provides active anterior cranial expansion via cranial springs. While SAC is well-described for sagittal craniosynostosis, its application in metopic craniosynostosis is less frequently described and comparative data evaluating postoperative cranial morphology remain limited. This study aims to compare treatment timelines and postoperative cranial shape between SC and SAC using measurements derived from 3D laser scans.
This IRB-approved, retrospective cohort study included pediatric patients who underwent SC or SAC for metopic craniosynostosis between 2021-2024 and completed helmet therapy. 3D laser scan data were collected at helmet initiation and completion. Metrics included anterior cranial volume and anterior-posterior volume ratio (APVR). Normally distributed variables are presented as mean±SD and compared using t-tests; non-normal variables are summarized as median [IQR] and analyzed with Wilcoxon Rank Sum tests.
Ten patients (5 SAC, 5 SC) were included in this study. There was no difference between SAC and SC for age at diagnosis (46.4±45.6 vs 63.4±29.5 days, p=0.5) or age at surgery (134.0±28.2 vs 110.4±10.7 days, p=0.12). For SAC patients, springs remained in place for 80±8.5 days before removal. At helmet initiation, anterior volume in the SAC group was 435.5±66.6 mm3 and 328.4±91.8 mm3 in the SC group (p=0.07). After completion of helmet therapy, anterior volume was 481.1±48.5 vs 414.1±67.2 mm3 (p=0.11) for SAC and SC, respectively. Initial APVR was 0.95 [0.92, 0.97] for SAC and 0.91 [0.90, 0.94] for SC (p=0.3), with final values of 0.961±0.034 and 0.926±0.023, respectively (p=0.09). Helmet therapy duration was significantly shorted in SAC (97.8 ±48.3 vs 187.4 ±54.9 days, p=0.03), with no difference in total time from surgery to helmet therapy completion (199.4 ± 39.3 vs 184.8 ± 52.7, p=0.63).
Within the first year postoperatively, no significant differences were observed in anterior volume or APVR between SAC and SC. There is a trend toward greater anterior volume SAC patients even prior to helmet therapy completion. SAC resulted in significantly shorter helmet therapy duration. These findings suggest that SAC offers at least equivalent morphologic and cranial volume improvement and reduced reliance on prolonged orthotic therapy in metopic craniosynostosis.
-

Impact of Severity and Surgical Timing on Neurodevelopmental and Ophthalmologic Outcomes in Isolated Sagittal Craniosynostosis
Rachel Lee, Caroline Baker, Theresa Nguyen, Victoria Vespa, Morgan Lentz, John Girotto, and Anna Carlson
Publication Date: 5-8-2026
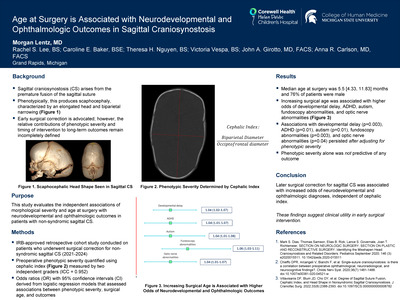
The influence of morphological severity and surgical timing on neurodevelopmental and ophthalmologic outcomes in sagittal craniosynostosis (CS) remains unclear. This study aimed to evaluate how cranial severity and age at surgery relate to these outcomes in patients with isolated sagittal CS.
A retrospective cohort study was conducted on 136 patients who underwent surgery for non-syndromic sagittal CS between 2012 and 2024. Morphological severity was quantified using cranial index measured by two independent graders (ICC = 0.952). Neurodevelopmental and ophthalmologic diagnoses were obtained from multidisciplinary clinic records. Odds ratios (ORs) with 95% confidence intervals (CIs) were derived from logistic regression models that assessed associations between cranial severity, surgical age, and each outcome. Continuous variables were non-normally distributed and reported as median [IQR].
Median age at surgery was 5.5 [4.33, 11.83] months and 76% of patients were male. Increasing surgical age was associated with higher odds of developmental delay (OR 1.04 [1.02-1.07], p=0.002) speech delay (OR 1.03 [1.00-1.05], p=0.03), ADHD (OR 1.04 [1.01-1.07], p=0.009), autism (OR 1.04 [1.01-1.08], p=0.01), fundoscopy abnormalities (OR 1.06 [1.03-1.11], p=0.001), optic nerve abnormalities (OR 1.04 [1.01-1.07], p=0.01), and strabismus (OR 1.03 [1.00-1.05], p=0.04). Associations with developmental delay (p=0.003), ADHD (p=0.01), autism (p=0.01), fundoscopy abnormalities (p=0.003), and optic nerve abnormalities (p=0.04) persisted after adjusting for severity. Severity alone was not predictive of any outcome.
Later surgical correction for sagittal CS was associated with increased odds of neurodevelopmental and ophthalmologic diagnoses, independent of cranial severity. These findings suggest clinical utility in early surgical intervention.
-

Emergency Preparedness in Michigan: Lessons from Hazardous Chemical Accident Data during 2021-2024
Sebastian Loonen, Jessica Park, Britton Michmerhuizen, Abby Shah, Emma Lindemann, Brianna Decker, Alex Ky, Daniel Bishay, Brian Lewis, and Jon Krohmer
Publication Date: 5-8-2026
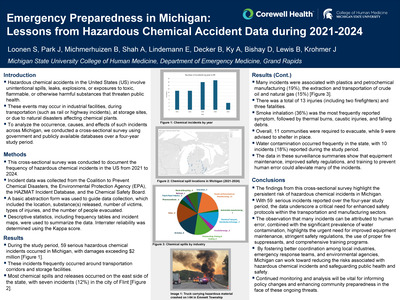
Hazardous chemical accidents in the United States (US) involve unintentional spills, leaks, explosions, or exposures to toxic, flammable, or otherwise harmful substances that threaten public health. These events may occur in industrial facilities, during transportation (e.g., rail or highway incidents), at storage sites, or as a result of natural disasters that affect chemical plants. To analyze the occurrence, causes, and effects of such incidents across Michigan, we conducted a cross-sectional survey using government and publicly available databases over a four-year study period.
This cross-sectional survey was conducted to document the frequency of hazardous chemical incidents in the US from 2021 to 2024. Incident data was collected from the Coalition to Prevent Chemical Disasters, the Environmental Protection Agency (EPA), the HAZMAT Incident Database, and the Chemical Safety Board. A basic abstraction form was used to guide data collection, which included the location, substance(s) released, number of victims, types of injuries, and the number of people evacuated. Descriptive statistics, including frequency tables and incident maps, were used to summarize the data. Interrater reliability was assessed using the kappa statistic.
During the study period, 55 serious hazardous chemical incidents occurred in Michigan, resulting in damages exceeding $ 2 million. These incidents frequently occurred around transportation corridors and storage facilities. Most chemical spills and releases occurred in the east side of the state with 7 incidents (13%) in the city of Flint. Many incidents were associated with plastics and petrochemical manufacturing (18%), the extraction and transportation of crude oil and natural gas (15%), and the transportation and storage of chemicals (6%). There was a total of 13 injuries (including two firefighters) and three fatalities. Overall, 11 communities were required to evacuate, while 9 were advised to shelter in place. Water contamination occurred frequently in the state, with 10 incidents (18%) resulting in contamination. The data in these surveillance summaries show that equipment maintenance, improved safety regulations, and training to prevent human error could alleviate many of the incidents.
This cross-sectional survey underscores the persistent risk of hazardous chemical incidents in Michigan, with 55 serious events reported over four years. These incidents, often linked to human error in transportation and manufacturing sectors such as plastics, petrochemicals, and oil and gas, highlight the need for improved equipment maintenance, stricter safety regulations, appropriate fire suppressants, and robust training. Strengthened coordination among industry, emergency responders, and environmental agencies, alongside continued monitoring, is essential.
-

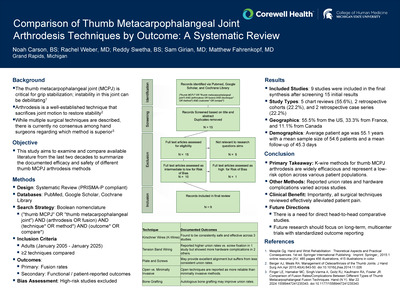
Nasal Regurgitation and Weight Trends Before and After Palatal Lengthening in Patients with Cleft Palate Related Velopharyngeal Insufficiency
Lasya Marla, Hamed Moshref, Samuel Girian, Elizabeth Bushong, Anna Carlson, and John Girotto
Publication Date: 5-8-2026
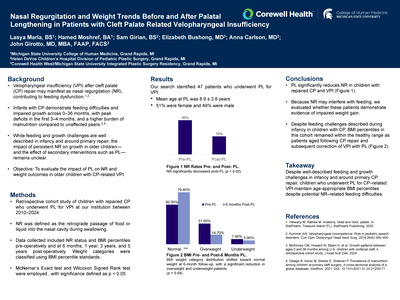
Individuals with cleft palate (CP) are more likely to face feeding and growth difficulties, which are often exacerbated by the presence of velopharyngeal insufficiency (VPI)/nasal regurgitation. Existing literature have explored short-term weight trends within the first 1-1.5 years of life; however, long-term BMI trends in older patients remain underinvestigated. Palatal lengthening (PL) aims to improve VPI, including nasal regurgitation, but its effects on nutritional status are not well known. This study evaluates the impact of PL on nasal regurgitation and weight trends in patients with cleft palate related VPI.
A retrospective review was conducted on patients who underwent PL to correct VPI at a single institution between 2010 and 2024. The presence or absence of nasal regurgitation and BMI percentiles were collected both pre- and post- operatively. Particularly, BMI percentiles were analyzed at the 6-month, 1 year, 3 years, and 5 years post-operative time points. Wilcoxon Signed Rank test was used to analyze differences in BMI pre- vs post- PL. T-test and Wilcoxon Rank Sum test were used to compare BMI between nasal regurgitation groups.
Our study included 47 patients with a mean age of 8.87 ± 3.76 years old at the time of PL. Prior to PL, 36.2% of patients experienced nasal regurgitation, which reduced to 19.2% post-operation (p = 0.022). The average pre-operative BMI percentile was 50% [25%, 85%]. At 6 months, 1 year, 3 years, and 5 years follow-up the average BMI percentiles were in the healthy weight category: 48.3%, 33.5%, 35.0%, and 34.5%. Of significance, the proportion of underweight patients decreased 6 months post-operation (p = 0.046), but changes were not noteworthy beyond this point of follow-up.
PL significantly reduces nasal regurgitation amongst patients with cleft palate related VPI. The post-operative BMI improvements suggests that PL may facilitate weight normalization via a reduction in nasal regurgitation. Such changes underscore the role of PL in improving nutritional outcomes. Overall, a multidisciplinary approach is essential to cleft repair.
-

A Rare Case of Pediatric Bartonella Neuroretinitis
Katie McCarthy, Gabby Young, and Stephen Gunnink
Publication Date: 5-8-2026
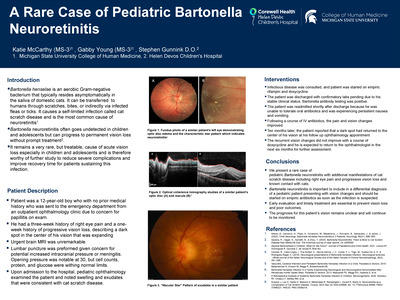
Bartonella henselae is an aerobic Gram-negative bacterium that typically resides asymptomatically in the saliva of its hosts, domestic cats. It can be transferred directly to humans through scratches or bites or indirectly via infected fleas or ticks. It causes a self-limited infection called cat scratch disease and is the most common cause of neuroretinitis1. However, Bartonella neuroretinitis often goes undetected in children and adolescents and can progress to permanent vision loss without prompt treatment2. It remains a very rare, but treatable, cause of acute vision loss especially in children and adolescents and is therefore worthy of further study to reduce severe complications and improve recovery time for patients sustaining this infection.
Patient was a 12-year-old boy who with no prior medical history who was sent to the emergency department from an outpatient ophthalmology clinic due to concern for papillitis on exam. He had a three-week history of right eye pain and a one-week history of progressive vision loss, describing a dark spot in the center of his vision that was expanding. He was urgently taken to MRI which was unremarkable. A lumbar puncture was preformed which was notable for an opening pressure of 30, although the CSF studies were unremarkable. Upon admission to the hospital, pediatric ophthalmology examined the patient and noted swelling and exudates that were consistent with cat scratch disease.
We present a rare case of pediatric Bartonella neuroretinitis with additional manifestations of cat scratch disease including right eye pain and progressive vision loss and known contact with cats. Bartonella neuroretinitis is important to include in a differential diagnosis of a pediatric patient presenting with vision changes and should be started on empiric antibiotics as soon as the infection is suspected. Early evaluation and timely treatment are essential to prevent vision loss and poor outcomes.
-

RA, You Take My Breath Away: Recurrent Pneumothorax in a Patient with Rheumatoid Arthritis Who was Weaned off Chronic Steroids
Samuel Miller, Melanie Mrozek, Robert Ocomen, Lara Hakim, Wahaaj A. Khan, and Maximiliano Tamae Kakazu
Publication Date: 5-8-2026
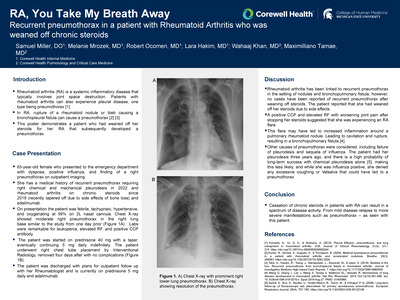
Rheumatoid arthritis (RA) is a systemic inflammatory disease that typically involves joint space destruction. Patients with rheumatoid arthritis can also experience pleural disease, one type being pneumothorax [1]. Pneumothorax is defined as the accumulation of air in the pleural space with collapse of the lung. This can occur in Rheumatoid Arthritis due to the rupture of a rheumatoid nodule or bleb, causing a bronchopleural fistula [2] [3]. We present a case of a patient who had weaned off her steroids for her rheumatoid arthritis that subsequently presented with pneumothorax.
A 65-year-old female with a history of recurrent pneumothorax requiring right chemical and mechanical pleurodesis in 2022 and RA on chronic steroids since 2019 (recently tapered off due to side effects of bone loss) and adalimumab. She presented to the emergency department with dyspnea after having a positive influenza test and a chest X-ray revealing right pneumothorax as an outpatient. On admission, she was febrile, tachypneic, hypertensive, and oxygenating at 99% on 2L nasal cannula. Laboratory results showed leukopenia, elevated rheumatoid factor (RF), and positive cyclic citrullinated peptide (CCP) antibody. Repeat chest X-ray showed moderate right pneumothorax in the right lung base, similar to the study completed as an outpatient the day before.
Rheumatoid arthritis has been linked to recurrent pneumothorax in the setting of rheumatoid nodules and bronchopulmonary fistula; however, no cases have been reported of recurrent pneumothorax after weaning off steroids. The patient reported that she had weaned off her steroids due to side effects. With her RA symptoms and inflammatory markers worsening after her taper, it is plausible that this taper may have led to her pneumothorax. In summary, weaning off chronic steroids in RA could lead to worsening of the disease and complications including pneumothorax.
-

Characterization of Shunt-Related Craniosynostosis in a Single Institution Pediatric Cohort
Macy Mitchell, Caroline Baker, Hamed Moshref, Samuel Girian, Casey Madura, and Anna Carlson
Publication Date: 5-8-2026
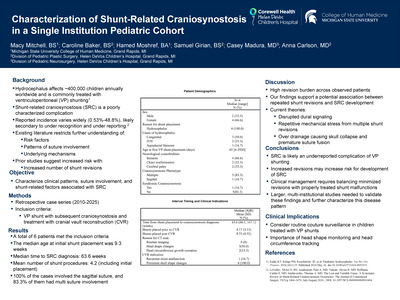
Shunt-related craniosynostosis (SRC) is a poorly characterized sequela of CSF diversion, with reported incidence varying significantly from 0.53% to 48.8%. This range likely reflects underreporting as suture fusion may be overlooked unless specifically studied. Current literature is restricted to a few case series, limiting analysis of risk factors and pathophysiologic mechanisms. Early data suggests that an increased number of shunt revisions as well as older age at first shunt insertion may be predictors of SRC development. In this study, we aim to expand upon the current body of knowledge by characterizing clinical patterns, suture involvement, and shunt-related factors associated with SRC observed at our institution. Additionally, we examine how our cases align with the current proposed mechanisms of SRC and highlight the diversity and complexity of this clinical entity.
This is a retrospective case series of patients treated with ventriculoperitoneal (VP) shunting followed by cranial vault reconstruction (CVR) for post-shunt craniosynostosis diagnosed between 2010-2025. Data were collected on the etiology of hydrocephalus, neurological comorbidities, shunt characteristics, time of SRC diagnosis, involved sutures, and associated complications.
There were a total of 6 patients fitting the search criteria. 67% of the patients were female, 100% of the patients were White and 100% of the patients were non-Hispanic. The median age at initial shunt placement was 9.3 weeks. The median time of onset between initial shunt placement and craniosynostosis diagnosis was 63.6 weeks. Patients had a mean of 4.2 shunt procedures, (before vs after craniosynostosis surgery.) All patients had involvement of the sagittal suture and 83.3% of the patients had multi-suture synostosis.
The substantial revision burden observed in our cohort suggests a potential association between increasing numbers of shunt revisions and elevated risk of SRC. Efforts to minimize the number of shunt revisions - when clinically appropriate - may help reduce the risk of SRC. However, this must be carefully balanced against the dangerous consequences of an untreated shunt malfunction. Overall, routine suture surveillance in patients treated with VP shunts may aid in early detection and improve the reporting and management of SRC.
-

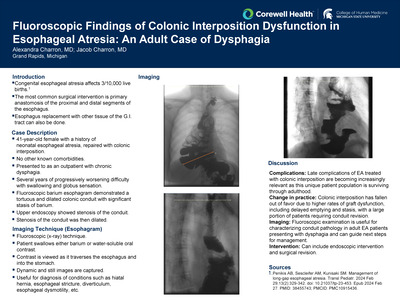
Continuity Counts: A Quality Improvement Initiative to Increase the Continuity of Care in an Academic Pediatric Residency Clinic
Geralyn Moody, Caroline Buckley, Katelyn Liu, Kristen Link, Christine Schafer, Miranda Hillard, Callie Kilpatrick, and kira Sieplinga
Publication Date: 5-8-2026
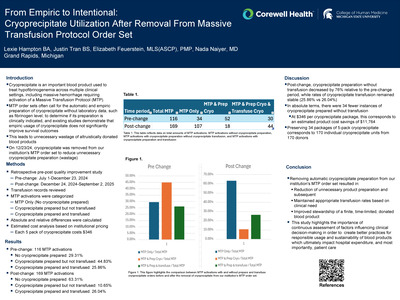
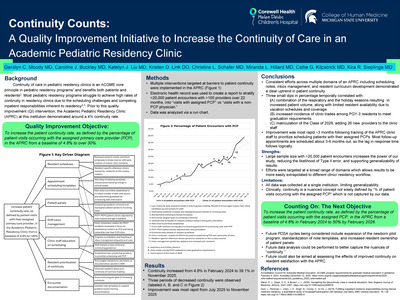
Continuity of care in pediatric residency clinics is an ACGME core principle in pediatric residency programs and benefits both patients and residents. Most pediatric residency programs struggle to achieve high rates of continuity in residency clinics due to the scheduling challenges and competing inpatient responsibilities inherent to residency. Prior to this quality improvement (QI) intervention, the Academic Pediatric Residency Clinic (APRC) at this institution demonstrated around a 4% continuity rate. This QI project aimed to increase the patient continuity rate, as defined by the percentage of patient visits occurring with the assigned primary care provider (PCP), in the APRC from a baseline of 4.8% to over 30%.
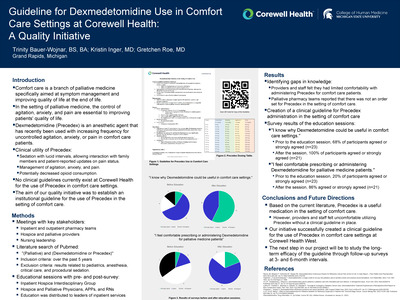
In response to the identification of low continuity rates, multiple interventions targeted at barriers to patient continuity were implemented in the APRC (Figure 1). The electronic health record was used to create a report to stratify >20,000 patient encounters with over >100 providers over 22 months, into "visits with assigned PCP" vs "visits with a non-PCP physician." A run chart was created to analyze data from February 2024 to November 2025.
An overall increase in continuity from 4.8% in February 2024 to 39.1% in November 2025 was achieved. Three periods of decreased continuity were observed, and improvement was most rapid from July 2025 to November 2025 (Figure 2).
Over the course of interventions targeting barriers to patient continuity in the APRC, the percentage of patient encounters with a PCP trended significantly upwards. With continued implementation and future PDSA cycles, the next goal is achieving 50% continuity by July 2026. Future cycles include expansion of the newborn pilot program, standardization of note templates, and increased resident ownership of patient panels. Future work will assess the effects of improved continuity on resident satisfaction with the Academic Pediatric Residency Clinic.
-

Hemorrhoidal Artery Embolization: A Retrospective Review of Outcomes and Cost Analysis
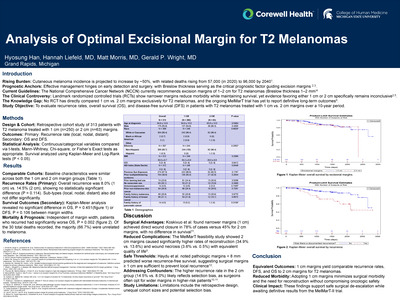
Matt Morris, Danielle Cadoret, Younes Jahangiri, Hannah Liefeld, Hyosung Han, James Ogilvie Jr., and James Morrison
Publication Date: 5-8-2026
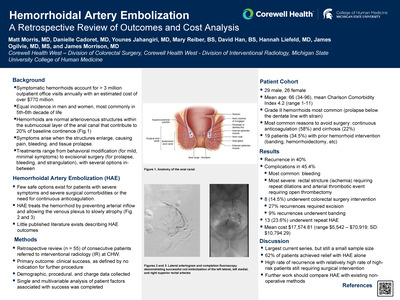
Limited options exist for hemorrhoidal disease in patients with severe comorbidities such extreme frailty, chronic pain, cirrhosis, or the need for continuous anti-coagulation. Hemorrhoidal artery embolization (HAE) has been proposed as a less invasive modality for treatment of patients who are unable to undergo banding or excision due to surgical contraindications, however data is limited. Our primary aim was to assess the efficacy of HAE compared to rates of recurrence and complications at a tertiary referral center to better understand which patients are most likely to benefit. Our secondary aim was to characterize charges associated with the procedure.
A retrospective review was performed on all patients referred for HAE to an Interventional Radiology department from 2020 - 2025. The primary outcome was clinical success, defined as resolution of hemorrhoidal bleeding, not requiring additional procedures. Data regarding demographics, clinical indication, pre- and post-procedural clinical status, outcomes, charges associated with the encounter, and the need for further hemorrhoid-related procedures were collected.
We identified 55 patients who underwent 69 instances of HAE. There were 26 female patients and 29 males with 35% (n=19) with grade 2 hemorrhoids. Mean age was 66, and mean Charlson-Comorbidity Index was 4.7 (range 1-11, mode 3). The most common surgical contraindication was continuous anticoagulation (58%, n = 32), followed by cirrhosis (22%, n = 12). Resolution of bleeding occurred after initial HAE in 62% of patients, however, 40% experienced hemorrhoidal recurrence. A second embolization was attempted in 13 cases, with clinical success achieved after one additional procedure in 62% (n = 8). Out of the 55 patients, 14.5% underwent additional procedures with colorectal surgery, most commonly excisional hemorrhoidectomy (n = 6). Two patients underwent banding and one is undergoing serial anal dilations. The average charges per HAE event was $17,574 (range $5,542 - 70,919).
Our results demonstrate that HAE is a safe option for patients with significant co-morbidities. In terms of resolution of bleeding, HAE was successful in most patients, however the procedure is also associated with significant rates of recurrence and need for repeat procedures. Future studies will be necessary to understand if this recurrence rate outweighs the risk associated with surgical intervention, as 15% of subjects still underwent surgery in this cohort. Additional studies can also compare charges incurred to traditional non-surgical options, such as sclerotherpies.
-

An Unlikely Culprit: Gastric Outlet Obstruction from an Ectopic Pancreatic Pseudocyst
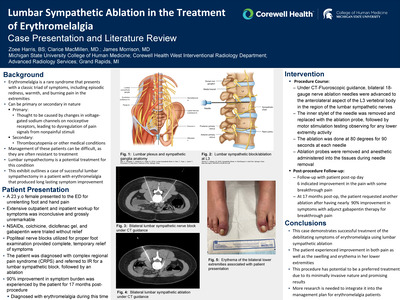
Erin Mueller, McKenzie Miller, and Gerald Wright
Publication Date: 5-8-2026
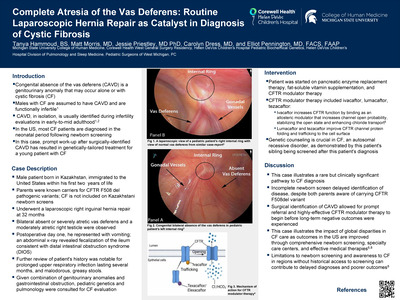
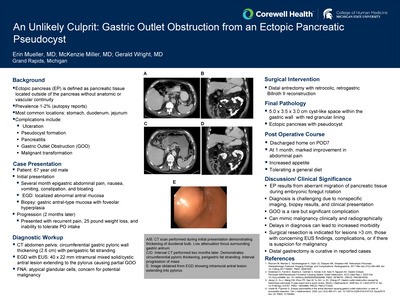
Ectopic pancreas (EP), also referred to as heterotopic pancreas, is defined as pancreatic tissue located outside the normal pancreas without anatomic or vascular continuity to the gland. Prevalence is 1-2% based on autopsy reports. EP is thought to result from aberrant migration of pancreatic tissue during embryonic foregut rotation and the stomach accounts for 24-38% of cases. Other common locations for EP include the duodenum and upper jejunum. While most cases are asymptomatic, complications can include ulceration, pseudocyst formation, pancreatitis, gastric outlet obstruction (GOO), or rarely malignant transformation. GOO caused by EP is especially rare with only a limited number of cases reported in the literature.
We report a case of a 67-year-old man who presented with progressive GOO from EP with pseudocyst formation, ultimately requiring surgical resection. He presented with several months of epigastric abdominal pain, nausea, vomiting, constipation, and bloating. Initial EGD revealed localized abnormal antral mucosa; biopsy showed gastric antral-type mucosa with features of foveolar hyperplasia. Two months later, he presented with recurrent pain, 25-pound weight loss, and an inability to tolerate oral intake. CT at this time revealed circumferential gastric pyloric wall thickening (2.6 cm) with perigastric fat stranding. Repeat EGD with EUS revealed a 40 x 22 mm intramural mixed solid/cystic antral lesion extending to the pylorus causing a partial GOO. FNA revealed atypical glandular cells.
Management of gastric EP depends on symptoms and degree of suspicion for malignancy. Asymptomatic lesions can be monitored, while resection is recommended for lesions > 3 cm, with concerning EUS features, or complications such as bleeding or obstruction. EP is an uncommon cause of GOO that should be included in the differential diagnosis of gastric submucosal lesions. Awareness of characteristic imaging and endoscopic features may raise suspicion and surgical resection is both diagnostic and therapeutic in symptomatic cases.
-

Acute Intraoperative Tension Pneumothorax after Reduction of a Traumatic Diaphragmatic Hernia During Laparoscopic Repair
Nicholas Mulder, Ken Dada, Alex Finn, and Nicholas Watson
Publication Date: 5-8-2026
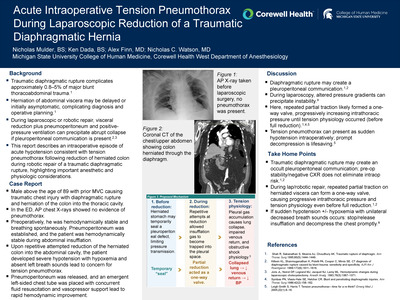
Traumatic diaphragmatic rupture can lead to pneumothorax if repaired laparoscopically. Herniation of abdominal viscera into the thorax may occlude communication between pleura and peritoneum at the site of trauma. Manipulation of the herniated tissue may lead to hemodynamic instability until the hernia is reduced and thoracoabdominal communication equalizes pressure.
A hemodynamically stable 92 year old male with traumatic diaphragmatic rupture and herniated colon into the thoracic cavity underwent robotic assisted laparoscopic reduction of the colon from the chest and repair of the diaphragmatic hernia. He was breathing spontaneously on supplemental oxygen preoperatively with adequate oxygenation. Intraoperatively the patient's abdomen was insufflated, he was ventilated with positive pressure, and remained hemodynamically stable. He was placed in steep reverse Trendelenburg to assist in visualization. The patient became hypotensive during attempted reduction of the herniated colon. Multiple vasoactive medications were given without significant effect, auscultation demonstrated absent left-sided breath sounds, and tension pneumothorax was suspected. Abdominal insufflation was immediately discontinued and a left chest tube was placed with return of stable blood pressure. The colon was then able to be reduced and the diaphragm repaired.
In patients with chest trauma and diaphragmatic rupture with herniated viscus, preoperative stability does not exclude pleural vulnerability when performing laparoscopic repair with abdominal insufflation. Manipulation of herniated tissue may act as a one-way valve during repair and may precipitate tension pneumothorax; prompt recognition, cessation of insufflation, and emergent pleural decompression are critical in this setting. In such cases thoracic decompression prior to insufflation with a thoracostomy tube is prudent.
-

Pregabalin for Severe Immunotherapy-Induced Pruritus: A Case Report
Kaladevi Nadarajan, Kayla Andres, and Gretchen Roe
Publication Date: 5-8-2026
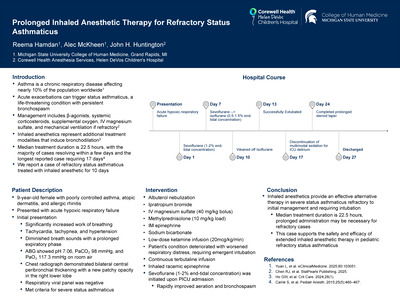
Immune-related cutaneous adverse events represent a significant clinical problem in cancer checkpoint inhibitor therapy, the most rapidly growing cancer treatment (1). Pruritus affects approximately 14% to 47% of patients undergoing treatment with immune checkpoint inhibitors, with 1% to 3% experiencing severe, widespread, and debilitating symptoms (2). This adverse effect significantly impacts quality of life yet remains poorly understood and often difficult to manage. Standard treatments such as topical agents and antihistamines offer limited relief, especially in cases of generalized pruritus. Systemic corticosteroids may provide transient benefit but are generally avoided for long-term use due to adverse effects.
60-year-old female with metastatic non-small cell lung carcinoma treated with carboplatin, pemetrexed, and pembrolizumab. She Initially developed itchy rash which somewhat responded to courses of prednisone. Then she developed generalized pruritus without rash. Multiple courses of prednisone, as well as trials of hydroxyzine, topical agents, and topical lidocaine, yielded minimal and temporary relief.
This case highlights the potential role of pregabalin as an effective therapeutic option for severe, immunotherapy-induced pruritus, particularly when standard treatments fail.
-

An Unusual Presentation of Neonatal Measles
Claudia Nadernejad, Daliya Khuon, Jennifer Jones, Mauli Patel, Jennifer Morse, Thrishika Balasuramanian, Tiffany Henderson, and Fatema Mamou
Publication Date: 5-8-2026
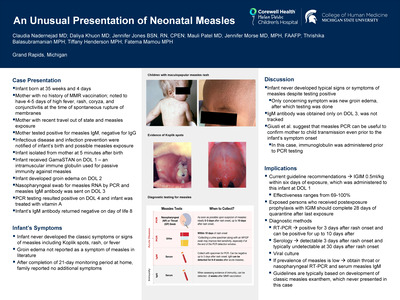
Measles is a highly contagious viral illness marked by classic symptoms of fever, rash, cough, coryza, and conjunctivitis. Measles rash typically presents 10-14 days after exposure. The best known protection against measles is the measles, mumps, and rubella vaccine. Current guidelines recommend administering IGIM 0.5ml/kg within six days of measles exposure. Additionally, guidelines for exposed persons who received postexposure prophylaxis with IGIM recommend 28 days of quarantine after last exposure. Our case presents the unique challenge of when PCR testing should be utilized in asymptomatic infants born to mothers with known measles exposure as guidelines for testing are largely based on development of the classic rash.
Patient was born at 35 weeks and 4-day gestational age to a G2P2 mother in her 20s via vaginal delivery. Mother had no history of MMR vaccination and received her prenatal care through a lay midwife. At the time of spontaneous rupture of membranes, she was noted to have 5 days of high fever and 4 days of rash, coryza, and conjunctivitis. Mother had recently traveled out of state with probable measles exposure. The infant was given GamaSTAN, an intramuscular immune globulin used for passive immunity against measles, on day of life (DOL) 1. Infant developed groin edema on DOL 2, which worsened from morning to evening. The swelling started at the penis and spread to the pubic area. On DOL 3, nasopharyngeal swab for measles RNA by PCR was sent to the state public health laboratory for testing. The infant was isolated from mother until DOL 4. On DOL 4, PCR testing returned positive for measles and the infant was started on vitamin A, 50 000 units per day for 2 days.
In this case, mother had confirmed exposure to measles at the time of delivery and the infant did not develop typical symptoms of expected measles infection. This does raise the question of when and via which method screening should be pursued. There are several ways to diagnose measles, including RT-PCR, serology, and viral culture. Interestingly, the guidelines for testing currently involve development of the classic measles exanthem, however, in our case, the infant never developed the typical rash. Instead, the only atypical symptom was groin edema.
-

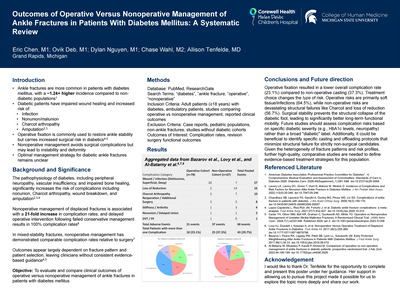
Male-Female Differences in Adult Patients Presenting to the Emergency Department with Fournier's Gangrene
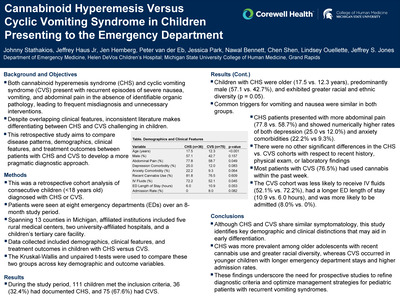
Andi Nations, Natalie Woodland, Sydney Hudock, Emily Hill, Jon Giolitti, Rachelle Pichot, Matthew Hysell, Nawal Bennett, Matthew Singh, and Jason Seamon
Publication Date: 5-8-2026
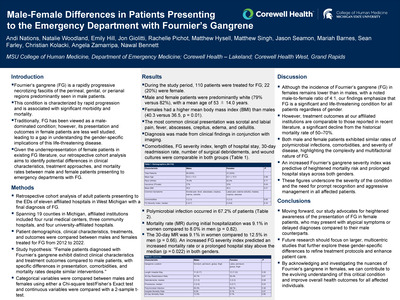
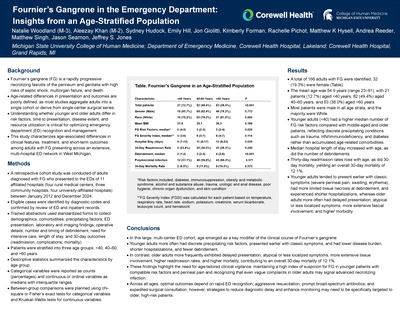
Fournier's gangrene (FG) is a rapidly progressive necrotizing fasciitis of the perineal, genital, or perianal regions, predominantly affecting men and poorly characterized in women. This study examined gender-specific differences in clinical features, treatment, and mortality among emergency department (ED) patients diagnosed with FG.
A retrospective cohort analysis was performed on adult patients presenting to the EDs of eleven hospitals across 19 Michigan counties from 2012 to 2022 with a diagnosis of FG. Institutions included four rural centers, three community hospitals, and four university-affiliated hospitals. Demographics, clinical characteristics, treatments, and outcomes were compared between male and female patients using Chi-square or Fisher's Exact tests.
A total of 110 patients were treated for FG; 22 (20%) were female. Mean age was 53 years, and most patients were white (79% of men, 82% of women). Females had a higher mean body mass index than males (40.3 vs. 36.5, p = 0.01). Common presentations included genital pain, fever, abscesses, crepitus, edema, and cellulitis. Polymicrobial infection occurred in 69% of cases. Both sexes had similar comorbidities, FG severity index, hospital stays, readmissions, and debridement numbers. Mortality during hospitalization was 9.1% in women and 8.0% in men (p = 0.82); 30-day mortality was 9.1% versus 12.5% (p = 0.66). Higher FG severity predicted greater mortality or prolonged hospitalization (p = 0.022).
FG incidence remains lower in women (male-to-female ratio 4:1), but outcomes between genders were comparable and reflect markedly improved survival over historical rates.
-

Successful Treatment and Suppression of Uncommon and Highly Morbid, Cladophialophora Bantiana Cerebral Phaeohyphomycosis.
Logan Neuhauser, Hannah Bray, and Joshua Donkin
Publication Date: 5-8-2026
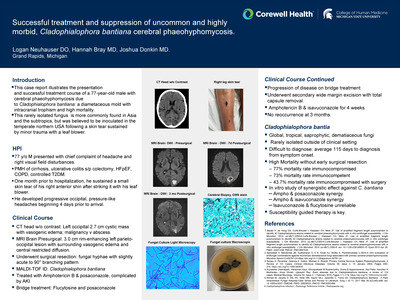
This case report attempts to illustrate the presentation and successful treatment course of a 77-year-old male found to have brain parenchymal abscess secondary to Cladophialophora bantiana, a diametaceous pigmented mold with intracranial trophism, known to have high mortality. This fungus is more commonly found in Asia and the subtropics, but was believed to be inoculated in the temperate northern USA following a skin tear sustained by contact with a leaf blower.
The patient presented for evaluation of lightheadedness, visual perceptual disturbances with seizure after arrival. MRI demonstrated a rim enhancing 3.0 x 2.6 x 3.0 cm left parieto-occipital lesion with central restricted diffusion concerning for a complex fluid collection. He underwent left occipital craniotomy and resection yielding a gray-mucinous material with cultures positive for cladophialophora bantiana as well as cutibacterium acnes.
-

Characterizing Aspirin-Only Brain Injury Guidelines Class 3 Patients Requiring Operative Neurosurgical Intervention
John Pardington, Jeremy Mormol, Nicholas Watson, and Alistair Chapman
Publication Date: 5-8-2026
The Brain Injury Guidelines (BIG) are a risk-stratification framework that categorizes patients with traumatic intracranial hemorrhage (ICH) into three tiers of increasing severity (BIG 1-3) based on various clinical and radiographic risk variables, with the most severe category designated BIG 3. Under the BIG, all patients taking aspirin are classified as BIG 3 regardless of other clinical variables. Anecdotally, physicians at our institution have observed that patients categorized as BIG 3 solely due to aspirin use generally experience favorable outcomes versus other BIG 3 patients. However, a small subset of these patients at our institution required invasive neurosurgical interventions (NSI). Our study aims to characterize this population and evaluate risk factors for neurosurgical intervention in these patients classified as BIG 3 solely due to aspirin use.
We conducted a retrospective single-center observational study of 36 adult traumatic ICH patients who met criteria for BIG 3 solely on the basis of aspirin use and underwent a neurosurgical intervention for management between 2020 and 2023. Clinical, demographic, radiographic variables, and operative procedures performed were extracted from the electronic medical record. Hemorrhage type, chronicity, location, and cerebral atrophy were obtained from radiology reports. NSI was defined as craniotomy, craniectomy, Burr hole, or placement of bedside intracranial pressure monitors or ventriculostomy drains. Statistical analysis was not performed due to the limited population size and our goal of characterizing this population.
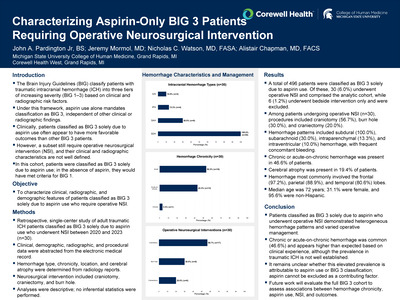
36 patients met the inclusion criteria. 30 patients (83.3%) underwent NSI in the operating room while 6 (16.7%) underwent NSI only at the bedside. Operative NSI involved craniotomy (56.7%), burr hole (30.0%) and craniectomy (20.0%). Hemorrhage patterns were subdural (94.4%), subarachnoid (41.7%), intraparenchymal (19.4%), and intraventricular (19.4%), with frequent concomitant hemorrhages. 15 patients (41.7%) suffered a chronic or acute-on-chronic bleed. Cerebral atrophy was noted in 7 (19.4%). Hemorrhage location was frontal (97.2%), parietal (88.9%), and temporal (80.6%) lobes. Compared with the overall cohort, patients requiring NSI were younger (median 72 vs 78 years), less often female (31.1% vs. 44.6%), and had similar ethnicity.
BIG 3 patients solely due to aspirin who underwent NSI demonstrate heterogeneity in hemorrhage characteristics, varied operative management, and a 42% incidence of chronic component of hemorrhage. The literature does not define a baseline rate of pre-existing chronic ICH in acute traumatic ICH, though this is very high compared to the expert radiologists we queried. It is unclear if this finding is unique to aspirin use or BIG 3 patients. Future work will evaluate the full BIG 3 cohort to assess associations between chronic hemorrhage, aspirin use, NSI, and outcomes.
-

Utilization of Ultrasound for Rapid Diagnosis and Management of Knee Septic Bursitis Overlayed with Purulent Cellulitis: A Case Report
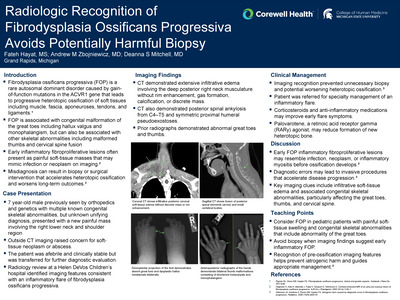
Matthew Park and Rebecca Loney
Publication Date: 5-8-2026
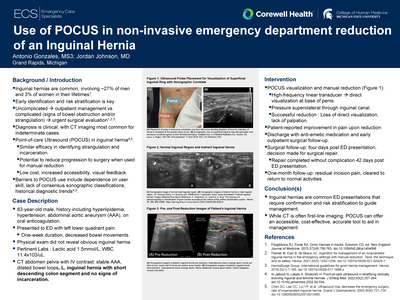
Prepatellar bursitis is a common cause of anterior knee pain and swelling and may present with erythema, warmth, and limited motion. When infection is present, distinguishing septic bursitis from cellulitis or septic arthritis can be clinically challenging. Aspiration and culture of bursal or joint fluid remain the diagnostic gold standard; however, overlying cellulitis and concern for deeper spread of infection may limit the safety of these procedures. Point-of-care ultrasound (POCUS) is increasingly recognized as a rapid, noninvasive imaging modality in the emergency setting that allows visualization of superficial bursae, adjacent soft tissues, and joint spaces. This case demonstrates the critical role POCUS has in guiding diagnostic and procedural decision-making in suspected septic bursitis, particularly when aspiration is relatively contraindicated. This case highlights the use of
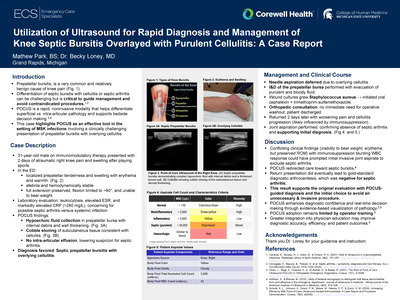
A 31-year-old man with a history of ulcerative colitis on immunomodulatory therapy presented to urgent care with two days of right anterior knee pain and swelling following recreational soccer. He denied direct trauma and was afebrile but unable to bear weight, prompting referral to the emergency department. Examination revealed warmth, erythema, and swelling localized to the prepatellar region with preserved knee extension and limited flexion. Laboratory studies demonstrated leukocytosis, elevated erythrocyte sedimentation rate, and markedly elevated C-reactive protein. Bedside musculoskeletal ultrasound revealed a hypoechoic fluid collection within the prepatellar bursa with internal debris and surrounding soft tissue changes consistent with cellulitis, without evidence of intra-articular effusion. These findings supported a diagnosis of septic prepatellar bursitis with overlying cellulitis and reduced concern for septic arthritis.
This case demonstrates how point-of-care ultrasound can rapidly distinguish septic prepatellar bursitis from septic arthritis and cellulitis in an immunosuppressed patient with acute knee swelling. By confirming bursal involvement and excluding intra-articular effusion, POCUS directly guided safe procedural decision-making and avoided unnecessary arthrocentesis. Early integration of ultrasound into the evaluation of musculoskeletal infections can improve diagnostic confidence, optimize management, and support timely, patient-centered care.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.