


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-

Effect of Nurse Driven Thirst Protocol on Perception of Thirst in ICU Patients
Trevor Beerer, Miranda Berisha, Ian Cangemi, Lauren Curran, Nicholas Elgert, Nicholas Fenchak, Jacob Hendee, Chloe Konopitski, Danielle Lafata, Randy Rofa, Courtney R. Rogers, and Kandise Watkins
Publication Date: 5-6-2026
Thirst is increasingly recognized as a significant yet often underassessed symptom among critically ill patients in the intensive care unit (ICU). Observational research indicates that thirst occurs in approximately 70–76% of ICU patients, with moderate to severe intensity levels commonly reported, making it one of the most prevalent discomforts experienced during critical illness (Negro, 2021). Factors such as fluid restrictions, mechanical ventilation, diuretic use, and limited access to oral hydration contribute to both the development and persistence of thirst in this population (Negro, 2021). Beyond physical discomfort, qualitative studies show that untreated thirst can lead to feelings of anxiety, distress, and powerlessness, negatively impacting patients’ overall ICU experience (Kjeldsen, 2017). Despite its high prevalence and impact, thirst is frequently overlooked in routine ICU care, highlighting a gap in symptom management (Negro, 2021). Emerging evidence suggests that structured, non-pharmacological interventions—such as oral cooling, menthol application, and early oral hydration—can significantly reduce both thirst intensity and distress compared to usual care (Liang, 2025). These findings support the potential value of implementing a standardized thirst protocol to improve patient comfort and outcomes in the ICU setting.
-

Improving CLABSI Prevention Through Central Line Education: A Quality Improvement Project
Lea A. Brenz
Publication Date: 5-6-2026
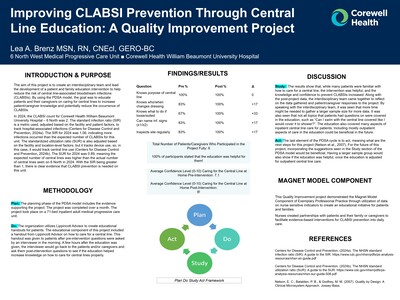
The aim of this project is to create an interdisciplinary team and lead the development of a patient and family education intervention to help reduce the risk of central line-associated bloodstream infections (CLABSIs). By using the PDSA model, the goal was to educate patients and their caregivers on caring for central lines to increase patient/caregiver knowledge and potentially reduce the occurrence of CLABSIs.
In 2024, the CLABSI count for Corewell Health William Beaumont University Hospital –6 North was 2. The standard infection ratio (SIR) is a metric used, adjusted based on the facility and patient factors, to track hospital-associated infections (Centers for Disease Control and Prevention, 2024a). The SIR for 2024 was 1.06, indicating more infections occurred than the expected number of CLABSIs for this unit. The standardized utilization ratio (SUR) is also adjusted based on the facility and location-level factors, but it tracks device use, so, in this case, it would track central line use (Centers for Disease Control and Prevention, 2024b). The SUR for 2024 was 0.89, meaning the expected number of central lines was higher than the actual number of central lines seen on 6 North in 2024. With the SIR being greater than 1, there is clear evidence that CLABSI prevention is needed on this unit.
-

Talk It Out: Using Daily Interdisciplinary Rounds to Elevate Nursing Communication
Casey Brooks, Gabrielle Jaworowski, and Maria Brown
Publication Date: 5-6-2026
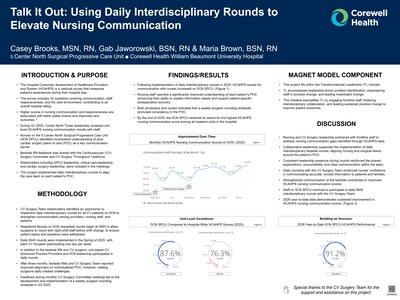
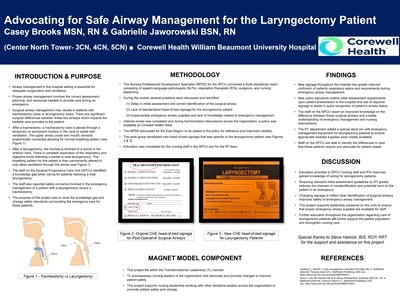
- The Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) is a national survey that measures patient’s experiences during their hospital stay.
- The survey includes 32 questions covering communication, staff responsiveness, and the care environment, contributing to an overall hospital rating.
- Higher scores in nursing communication and responsiveness are associated with fewer safety events and improved care outcomes. 2
- During Q1 2025, Center North Tower leadership reviewed unit-level HCAHPS nursing communication results with staff.
- Nurses on the 5 Center North Surgical Progressive Care Unit (5CN SPCU) identified inconsistent understanding of post-cardiac surgery plans of care (POC) as a key communication barrier.
- Bedside RN feedback was shared with the Cardiovascular (CV) Surgery Committee and CV Surgery Throughput Taskforce.
- Stakeholders including SPCU leadership, critical care leadership, and cardiac surgery leadership, were included in the meetings.
- This project implemented daily interdisciplinary rounds to align the care team on each patient’s POC.
-

Low-Cost Wellness Interventions to Reduce Nurse Stress on a High-Acuity Unit
Alaina Capoccia, Sarah Eib, Heather Gutpell, Danielle Saleh, and Kathleen Bajorek
Publication Date: 5-6-2026
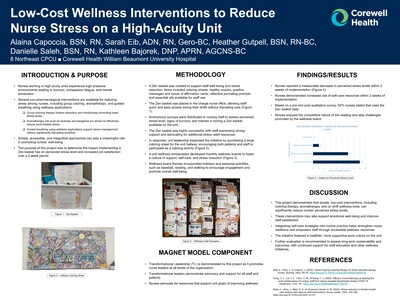
- Nurses working in high acuity units experience high-pressure environments leading to burnout, compassion fatigue, and mental exhaustion.
- Several non-pharmacological interventions are available for reducing stress among nurses,includinggroup coloring, aromatherapy, and guided breathing using wellness applications.
❑ Group coloring therapy fosters relaxation and mindfulness promoting lower stress levels.
❑ Aromatherapy oils such as lavender and bergamot are shown to effectively reduce work-related stress.
❑ Guided breathing using wellness applications support stress management without significantly disrupting workflow.
- Simple, accessible, and integrative approaches can play a meaningful role in promoting nurses’ well-being.
- The purpose of this project was to determine the impact implementing a Zen basket has on perceived stress level and increased job satisfaction over a 2-week period.
-

Inhale confidence: Keep Your Lungs Open & Moving
Meredith Chesney, Sumerlyn Bellthomas, and Andrew Veridiano
Publication Date: 5-6-2026
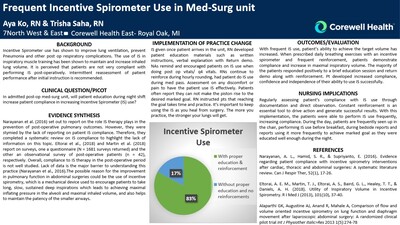
Atelectasis is a concern for all patients; not limited to pre-and post-surgical patients. An issue that we as nurses have noticed is the lack of incentive spirometer (IS) education for patients admitted to 5NE. In our post-operative patients’, acute/chronic pain and limited mobility serve as factors that prevent full ventilation and perfusion of the lungs. One of the ways wemitigate ventilation and perfusion deficits for our patients, is the use of the IS. There are many variables that still influence and limit the patients’ use of the IS therapy. Variables include; poor education, inaccessibility of the device, and lack of cooperation from the patient. As nurses, our main priority is to advocate for our patient's health. When providing education to our patients, nurses need to highlight the benefits of utilizing proper IS techniques to help prevent further pulmonary deterioration.
Incentive spirometer is used in lung expansion therapy tomaintainalveolar patency and improve pulmonary volumes. A 2021 study by Toor et al., focused on patients with severe respiratory disease who have a baseline cough. IS education and instructions were provided to the patients in the study. Results showed 16% increase in maximal inspiratory volume over a span of 30 days when prescribed daily breathing exercises with an IS. Supporting research concluded by Bilyyet al. (2020)indicatingthat pre-operative incentive spirometer education and IS exposure ensures better compliance with post-operative treatment andappropriate use. It was noted length of stay also significantly reduced in ICU patients who practiced deep breathing and incentive spirometer use (Hatice et al., 2025). In more recent research inpatients who underwent open heart surgery who were exposed to incentive spirometer use continued to have decreased hospitalizations and increased post surgical outcomes (Hatice et al., 2025). The evidence of benefits created with the integration of IS use for hospitalized patients, has made it imperative to implement better education to increase compliance on IS use for patients on the 5 NE.
-

Sleep Smarter, Heal Faster!
Shelby Conrad, Monica Tuchlei, Taion Goode, and Kristin Lerchenfeldt
Publication Date: 5-6-2026
Medical Surgical patients often experience pain, anxiety, and disruptions from hospital environments. This often leads to poor sleep quality. Implementation of a sleep hygiene protocol has shown to enhance patient’s recovery and healing process. When patients sleep well, they are more likely to engage in their treatment plan and report higher satisfaction with care. The current, most used method of resolving patients poor sleeping qualityis sleeping pharmaceuticals.
Research shows that poor sleep in hospitalized patients is linked to delayed healing, increased pain, and lower satisfaction. Studies like Beswicket al. (2023) and Dacharyaet al. (2024) support non-pharmacological strategies-such as environmental changes and care clustering-to improve sleep quality. Andrade (2021), highlights the risks of sedative use when caring for patients at risk for hospital acquired delirium and falls. Overall, evidence supports that simple, nurse-led sleep hygiene interventions can enhance rest, recovery, and patient experience in a safe and effective manner.
-

Pressure Injury Prevention in the ICU Setting
Morgan Dempster and Elizabeth Roman
Publication Date: 5-6-2026
Pressure injuries occur when a patient stays in the same position in bed for an extended time period. The heaviest and boniest parts of the body, commonly the back of the head, spine, sacrum, and heels, push down on the bed leading to skin breakdown. The easiest way to combat this breakdown is by turning patients every two hours, something that the nurses on this unit have complete control over. Cox et al., (2022) states that it is four times more likely for patients admitted to the ICU to develop pressure injuries than other hospital units. Much of this can be attributed to the fact that majority of ICU patients are unable to move themselves in bed due to intubation, sedation, or high acuity. Pressure injury risk is often measured by the Braden Scale, which consists of mobility, activity, sensory perception, skin moisture, nutrition, and friction/shear (Labeau et al., 2021). Patients with low Braden Scores should indicate to nurses that they will require more attention and care when it comes to skin.
-

Hourly Rounding To Reduce Adult Fall Risk
Yzabel Enojas, Lia Olowniuk, and Tori Ottenbacher
Publication Date: 5-6-2026
Falls are a major safety concern in adult inpatient settings, with over 20% of people sustaining moderate-to-severe injuries, such as hip fractures or head trauma (Hicks, 2015). Injuries sustained from falls significantly increase healthcare costs due to prolonged hospital lengths of stay and the utilization of numerous, and often costly, resources (Hicks, 2015). The current standard of nursing care to prevent falls in hospital settings involves ensuring that patients have access to the call light with their belongings within reach. However, even with these prevention interventions, falls are still occurring. Hourly rounding (HR) is the proactive and intentional process whereby a member of the nursing staff performs rounds on every patient every hour to identify and address the patients’ needs (Sun et al., 2020). Implementing HR as an intervention will ensure patient safety and support patients’ needs in their designated environment.
Evidence-based practices consistently demonstratesthat structured hourly rounding reduces patient falls and promotes safety. Sun et al. (2020) shows that incorporating hourly rounding with bedside shift reports reduce fall rates. It’s crucial to include that each patient has their own unique needs therefore ensuring timely attention to patient needs should also be considered. Glineret al. (2021) reported that clear nurse-patient communication, nurse to nurse communication and frequent rounding are associated with a reduction of fall rates. For example, it’s important to walk into patient rooms and ensure their bed alarm is on. If a patient needs or is asking for something specific, it’s crucial to address patient needs by informing their primary nurse. Additionally, Fridman (2019) emphasizes educating nurses on hourly rounding with meaning makes a difference within patient safety. Evaluatingpatient outcomes and satisfaction can help this practice stay up to date. Similarly, Hicks (2015), in an integrative review, concluded that systematic rounding by proactively addressing pain, positioning, toileting and person items in reach reduces fall events. In conclusion, these studies implement the importance of purposeful hourly rounding is a definitive, evidence-based practice for reducing fall rates in hospital care settings.
-

Music Therapy for Restlessness and Agitation in End-of-Life Care
Brandi Forris
Publication Date: 5-6-2026
Music therapy is recognized as a complimentary alternative medicine (CAM) and is used with increasing frequency in the treatment of those during the dying process. There is empirical research literature supporting the use of music therapy in palliative/end-of-life care dating back to the 1970’s. Music therapy programs are implemented in hospice and palliative care, with more and more patients and families having access to the provided services. Creating an evidence base for music therapy will assist clinicians in establishing best use practices in end-of-life care.
-

Separation and Color-Coding labels of Telemetry Monitors: -Exemplary Professional Practice A Strategy to Reduce False Rhythm Events in Cardiac Progressive Care
Mirna Khorka
Publication Date: 5-6-2026
Implementing this change is important because an incident occurred on CPCU where the wrong box was connected to the wrong patient in a shared room. This error led to inaccurate rhythm interpretation placing both patients at risk for delayed or inappropriate interventions. By evaluating whether separating TMS boxes and adding color coded stickers reduces false rhythm readings, improve monitoring accuracy, prevent adverse patient safety, and strengthen trust within our telemetry system. Currently, the boxes are stored together in centralized locations in shared rooms with yellow color sticker labels on all. When a new patient is admitted or when telemetry needs to be reapplied, staff retrieve a box from the shared TMS doc location and connect it to the patient. Because patients are frequently placed in shared rooms, there is an increased risk of mistakenly assigning the wrong monitor box to the wrong patient.
-

Oral Care Visual Cue and Education to Improve Oral Care Compliance
Samuel Lico
Publication Date: 5-6-2026
2-East is a Cardiovascular Surgical Intensive Care Unit (CVSICU), that specializes in the care of patients requiring cardiovascular surgical interventions, in addition to patients requiring general surgical interventions. With the primary patient population under-going open-heart surgeries, many of these patients come back to the CVSICU on ventilator support. With many surgical patients requiring prolonged ventilator support, ventilator-associated pneumonia (VAP) is a serious complication that can occur in critically-ill patients as a result ofpoor oral hygiene. Although not all patients require ventilator support, patients in this setting are often incapable of performing their own oral care and are dependent on nurses for their oral care needs. Our current unit practices require oral care with chlorhexidine once a shift and every two to four hours after that, or as needed. However, with the high acuity of our patient population and busy workloads, nurses often forget to stay on top of oral care practices. Therefore, implementing a visual cue reminder with education to be posted in patient rooms, above oral-care kits, can help narrow this gap in practice.
-

Fluid Balance Fundamentals: Optimizing Intake Documentation
Kimberley Mannering, Peter Laframboise, and Renee Metropoulos
Publication Date: 5-6-2026
A patient's intake is critical for ensuring patient safety and enhancing clinical outcomes. In the hospital setting, all patients have either a diet order or are NPO (nothing by mouth) with IV fluids infusing.7NW as a whole unit, is incredibly good at tracking outputs for patients (ex. urine, drains, and ostomy output).An area for opportunity is tracking intake, specifically PO fluid intake. Charting IV fluid intake can be easily done as Epichelps make thosecalculations. It is more difficult to accuratelymonitor PO fluid intake in patients, especially with melted ice or abandoned, lukewarm water cups in their rooms.Whileit may not seem important and just a small part of the patient’s day to day life in the hospital, PO fluid intake is crucialfor getting a whole picture of the patient’s overall health. More specifically, it is vital information if patients are on fluid restrictions or a restricted diet.
There are often situations when a patient'sdiet order is advanced and their IV fluid rate decreased or discontinued; but they are not adequately taking in a lot of oral fluid. Dehydration can become a real problem, particularly in our elderly populations. Elderly patients are more prone to dehydration due to lower overall percentage of fluid in the body, decreased thirst, and reduced kidney function (Cohen et. al, 2021). A 2023 systemic review found that in both, med/surg and ICU, settings patients oral fluid intake was often incorrectly charted or simply not charted at all (Leinum et. al., 2023). 7NW is primarily a surgical unit (ex. urology, colorectal, bariatric, etc.). For patients who are scheduled for surgery typically have an order for IV fluids the night prior to surgery as the patient is NPO. Once in surgery they get more intra-operative IV fluids to keep a fluid balance. After surgery,the patient will come back on the unit with continuedIV fluids infusing and usually some kind of oral diet. A 2020 study of postoperative patients found that patients receiving more than 20mL/kg/day of fluids from both IV and PO sources had an increased mortality rate than those who did not (Sim et. al., 2020). It is clinically important to maintain a fluid balance and have good documenting skills.
Does writingdates and times on water cups for patients in an inpatient setting improve accurate charting of intake and help improve the overallpicture of the patient’s health?
-

Knowledge and Performance with Crash Cart Education
Nicole Mason, Tina Eid, and Katelyn Sparks
Publication Date: 5-6-2026
Emergency crash carts provide life-saving supplies, medications, and equipment used during medical emergencies. Lack of proper education on emergency response protocols and crash cart equipment can result in decreased patient outcomes and an anxiety-inducing experience. As a result, it is crucial nurses feel confident and can provide optimal care in a timely manner. The desire outcome of this project is to enhance confidence in crash cart knowledge, ultimately improving competency and response time during emergency situations. The goal of this project is to see what percentage of nurses find increased crash cart education helpful during codes.
-

Fluid Resuscitation s/p Open Heart CABGs vs Valves
Samantha Nadolski
Publication Date: 5-6-2026
-
In CABG (coronary artery bypass graft) and valve patients, fluid shifts occur post operatively due to inflammation of the tissues resulting in leaky blood vessels causing hypotension or low blood pressure.
-
Colloids can be blood products, such as human albumin solution and fresh frozen plasma, or they can also be synthetic large molecules which are not able to distribute across vascular barrier such as gelatins, dextrans, and hydroxyethyl starches. (Post operative fluid management, 2015)
-
In this study, data was collected from a total of 22 patients in the SICU at CHE over a two week time span tracking hemodynamics and pressor/inotrope use at the time of albumin administration within the first 24 hours post-op. The goal is to compare CABG and valve patients fluid needs after surgery.
-
-

Alternative Interventions for Confused Patients
Elise Pechler and Aram Ferhadson
Publication Date: 5-6-2026
An Evidence-Based Practice (EBP) project is included in nurse residency programs to bridge the gap between academic theory and clinical practice. It empowers new nurses to enhance patient care quality, build critical thinking skills, increase professional confidence, and meet organizational standards like Magnet designation.
Keeping patients healthy and safe is one of our top priority as nurses. However, this can become a challenge when patients become confused or agitated as they can risk harming themselves by pulling out lines or falling. Most nurses are familiar with the use of bed alarms, safety sitters and restraints for hospitalized patients who are suffering from cognitive impairment, delirium, suicidal ideation, or another behavior-altering conditions. The goal of this project was to use less restrictive measures to keep patients safe as well as inform fellow nurses of available resources.
-

Clean, Safe, Ready: A Quality Improvement Approach to Reusable Equipment
Reagan Pozdol, Patricia Sierra Delgado, and Lindsay E. Colby
Publication Date: 5-6-2026
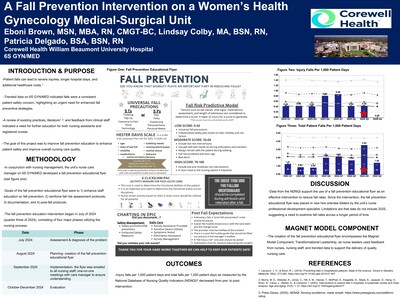
Research has shown that reusable hospital equipment can harbor microorganisms and bacteria especially when proper cleaning practices are not used (Browne et al., 2024). Improving the cleaning and disinfection of shared medical equipment significantly reduces hospital acquired infections (HAIs) underscoring the crucial role of cleaning in improving patient outcomes. Hospital systems, including Corewell Health, have policies outlining routine cleaning practices for reusable equipment. The goal of this quality improvement (QI) project is to improve knowledge of the proper (per policy) cleaning practices for reusable equipment on 6 South GYN/Medical.
A 2018 Australian study measured the amount of Colony Forming Units (CFUs) on blood pressure cuffs after uses, and again after cleaning to examine the effect disinfection had on the amount of CFUs grown. The results showed that after a single use of the cuff, bacteria grew between 51-100 CFUs, considered a moderate amount of growth. Overall, the study demonstrated that properly cleaning the cuffs significantly reduced the number of bacteria formed, suggesting cleaning between uses should be considered standard (Zimmerman, et al., 2018).
Another study examined how clinical nurses (CNs) self-reported how often they cleaned their stethoscopes between patients pre and post an educational intervention. The study found that pre-education, only 23.7% of CNs reported cleaning their stethoscopes between patients. Post-education findings were that 52.8% of CNs self-reported cleaning their stethoscopes between patients, a 29% increase (Guler, et al., 2024).
Third, Browne et al. (2024) examined 10 units within the same hospital over 36 weeks to evaluate their cleaning policies. Their study showed that when staff was educated on cleaning policies and implemented policy into practice, the prevalence of hospital acquired infections dropped from 14.9 -9.8%.
-

Improving Nurse Confidence in Emergency Response Situationsv
Paige Skorupski, Kathleen Bajorek, Samantha Start, and David Godell
Publication Date: 5-6-2026
- Prompt recognition of acute patient deterioration is essential, as timely intervention can mean the difference between recovery and further decline.
- Nursing experience varies widely, from new graduate nurses with less than one year of practice to highly seasoned nurses. These experience levels directly influence confidence, clinical reasoning, and the ability to recognize and respondto emergent events.
- Evidence demonstrates that simulation-based education like mock codes and rapid response drills enhance clinical competence, prompt critical thinking, and support strong team communication.
- Despite strong evidence to support simulation-based learning, many units still lack a structured ongoing program.
- Nurses are often the first to identify acute patient status changes, including arrhythmias, respiratory distress, chest pain, or early indicators of cardiac arrest.
- Targeted simulation training may improve nurse confidence during acute events, thereby indirectly supporting patient safety in high-acuity situations.
- This purpose of this project was to evaluate the impact of mock emergency response scenarios on nurse confidence in recognizing acute changes among patients on a cardiac progressive care unit.
-

Promoting Accuracy in Charting on Titratable Medications in the CVSICU
Elizabeth Sterner
Publication Date: 5-6-2026
Due to the crucial nature of the titration of blood pressure and sedative medications for high-risk instability in cardiovascular patients, it is important that nurses use the titration indicators such as The Richmond Agitation-Sedation Scale (RASS) and target systolic blood pressure (SBP) or mean arterial pressure (MAP) set in place by the provider to accurately and correctly reflect changes in patient response to achieve the desired therapeutic effects. Not only does having these tools in place ensure accuracy in charting for nurses, but it also allows for the doctors and the Advance Practice Providers (APP) to further make decisions about patient care and hemodynamics based on responses to change in titrations. Two pertinent factors that the Joint Commission enforces for titratable medications and their rapid administration are time of completion of the charting block and the psychosocial parameters evaluated to determine the administration of titratable medications during the charting block(Medication Administration-Titratable Orders-Documentation During Rapid Titration | Hospital and Hospital Clinics | Medication Management MM. 2021). By following these evidence–based practices when titrating medications in the ICU, safety, effectiveness, and timely treatment is most attainable.
-

Outpatient Blood Transfusion Emergency Response
Sherri Tatu, Natalie Dennis, Alesia Jirjis, and Alex McGinnis
Publication Date: 5-6-2026
Background
Outpatient blood transfusions are increasingly performed in hospital-based short stay and outpatient infusion units. While transfusion reaction management is embedded within the Outpatient Blood Transfusion Order set, emergent clinical deterioration unrelated to transfusion reactions lacks a consistent and clear response pathway in the outpatient setting.
On 1 South Short Stay Unit (1S SSU), patients experiencing symptoms wuch as shortness of breath, hypotension, chest pain, stroke symptoms, or sepsis are unclear and inconsistent. Ordering providers are often off-site, and the current Rapid Response Team (RRT) response is outlined for Inpatient setting but limited to Basic Life Support (BLS) and transport only, without authority to stabilize patients on scene.
Purpose
To develop and implement an Outpatient Transfusion Emergency Response Protocol that empowers nurses and the Rapid Response Team to provide timely, standardized assessment, stabilization, and escalation, reducing risk and improving patient outcomes.
-

Family Involvement in Daily ICU Team Rounds
Abby Wozniak
Publication Date: 5-6-2026
In the ICU, families play a large role in decision-making because many patients in this population are unable to make medical decisions for themselves. When families are involved in patient care and are up-to-date on their loved one's condition, it is easier for family members to understand the plan of care and facilitate decision-making. Families spend a lot of time with their loved ones in the hospital. By scheduling a time to promote family attendance in daily ICU team rounding, families and patients will have overall higher satisfaction with care and better outcomes.
In Adult ICU patients, does family participation in daily ICU team rounds, compared to standard communication, improve their understanding of the patient's plan of care over seven days?
Over a week, nurses asked family members, either in person or over the phone, if they would like to be present during the ICU team's daily rounds. Some family members were unable to attend due to previous obligations. After the week of implementation, the nurses asked the family members to fill out a form rating their satisfaction and knowledge of the plan of care for their loved one on a scale of dissatisfied to very satisfied.
-

Implementing Bedside Shift Report Amongst Clinical Nurses and Nursing Support Staff
Olivia Anthony
Publication Date: 5-2025
Collaboration between nursing support staff (NSS) and clinical nurses (CNs) is crucial for the provision of safe, personalized, quality care (Beynon et al., 2021). Currently, CNs and NSS on the inpatient rehabilitation (IPR) unit are not required to formally give or receive report from each other.
It is estimated that NSS provide 80%–90% of direct care to rehabilitation patients (Aloisio et al., 2021). Without a formal handoff process, there is a potential for missed communication of important clinical concerns. For instance, if a patient requires scheduled bladder scanning, has a strict intake and output protocol, or has a goal to sit in a chair for a certain length of time, NSS may or may not be aware until the CN can verbally review specific patient care needs with them, setting clear goals for each patient. The lack of a formal reporting process often results in NSS not receiving report from CNs for hours, pushing these essential conversations into later in the shift, and sometimes, if emergent issues arise, not at all (Potter et al., 2010).
The aim of this quality improvement project was to explore the effectiveness of bedside shift report amongst clinical nurses and assigned nursing support staff to improve patient outcomes on the IPR Unit.
-

Promoting Bedside Shift Report to Improve Nursing Communication Scores
Kathleen Bajorek, Heather Gutpell, and Danielle Saleh
Publication Date: 5-2025
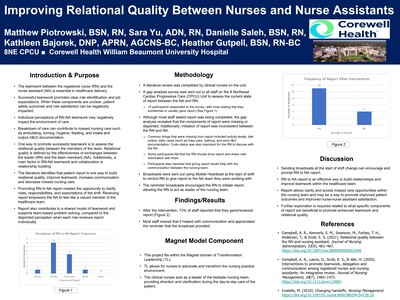
- • Bedside shift report (BSSR) has many benefits including improvement in safety and quality, preventing medical errors/adverse events, and improved patient and family experience scores.
- BSSR also improves accountability between nursing team members and improves nurse satisfaction.
- Hospital staff know the organizational culture and workplace functioning. However, patients and family are strangers to the environment and may not understand the system.
- Common barriers to BSSR include length of time to complete, perceived Health Insurance Portability and Accountability Act (HIPAA) violation, not wanting to disturb the patient, fear of change, and management of interacting with challenging families or patients.
- On 8NE Cardiac Progressive Care Unit (CPCU), compliance of BSSR was not meeting industry standards. Audits found that staff members would complete report at the desk in the nurse’s station or outside the patient’s room door.
- The 8NE Professional Nurse Council (PNC) and leadership teams coordinated together to brainstorm ways to increase compliance and comfort with BSSR.
- 8NE has been identified as a power unit with great opportunity to improve the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scored question “Nurses explained things understandably”. The goal of this project was to improve this unit score with a goal of 83.8% to 84.8%
- Nursing communication domain within the HCAHPS survey is the greatest influencer of the patient’s overall satisfaction score.
-

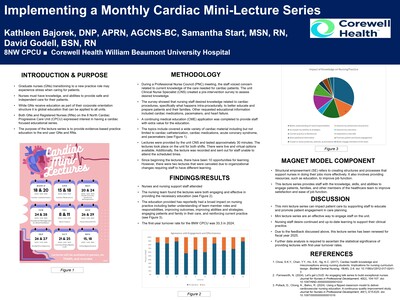
Implementing a Monthly Cardiac Mini-Lecture Series
Kathleen Bajorek, Samantha Start, and David Godell
Publication Date: 5-2025
- Graduate nurses (GNs) transitioning to a new practice role may experience stress when caring for patients.
- Nurses must have knowledge, and abilities to provide safe and independent care for their patients.
- While GNs receive education as part of their corporate orientation structure it is global education that can be applied to all units
- Both GNs and Registered Nurses (RNs) on the 8 North Cardiac Progressive Care Unit (CPCU) expressed interest in having a cardiac focused educational series.
- The purpose of the lecture series is to provide evidence-based practice education to the end user GNs and RNs.
-

Early Movement Leads to Patient Improvement
Lindsay Beard, Michelle Faetz, Kimberly Wesley, and Kristen Gawlik
Publication Date: 5-2025
As bedside nurses in the medical-surgical setting, we prioritize patient safety, strong critical thinking, and proper medication administration; but what about patient mobility? About 65% of older adults have a decline in their ability to ambulate or perform activities of daily living (ADL) post hospitalization (Pan, Y., Thiamwong, L., & Xie, R. (2023, January); which may lead to increased discharges to rehabilitation facilities and nursing homes as well as increased chances of hospital readmission.
The mobility pilot is a nurse-driven initiative that encourages nurses to ambulate and mobilize their patients' multiple times a day. Any form of mobility has been shown to improve aerobic capacity and shorten length of stay significantly for medical patients compared to conventional care (Hook, M., Dailey, M.S., Singh, M., Shneuker, D., Mitchell, L., Milligan, K., … Kelly, L. (2024). Our goal on 8 Center is to decrease the number of discharges to rehabilitation facilities by keeping patients active during their hospital stay, with the goal to return home.
To maintain and improve patient mobility, nurses must take an active role in the ambulation and movement of their patients. This includes utilizing the 6- clicks scores, an assessment tool derived from the Active Measure for PostAcute Care (AM-PAC) used to measure basic mobility, daily activity, and applied cognition to determine discharge disposition (Warren, M., Knecht, J., Verheijde, J., Tompkins, J. (2021) as well as implementing a mobility audit to keep track of which patients should be ambulating and how often. This quality improvement project aimed to show how nurses can reduce the amount of rehabilitation admissions by increasing ambulation and mobility, promoting patient autonomy, and preserving their ADL function.
-

Clinical Ladder Program: Participants and their Perspectives
Sarah Berry
Publication Date: 5-2025
Our health system offers a Clinical Ladder (CL) Program for Registered Nurses (RNs) that provides professional development opportunities and recognizes their knowledge, skills, efforts to support education, mentoring of new staff transitioning into practice, shared governance, and our ANCC Magnet Program® goals.
The program has been designed to encourage professional growth, improve the quality of care, and increase staff participation in activities that directly benefit each unit and site. The CL program has certain requirements and activities that must be completed within 12 months of signing a letter of intent (LOI) to complete the program. The ability to participate in the program is dependent on the RN’s manager’s approval.
Our health system has a CL committee which is tasked with evaluating applications as well as reviewing and updating the program as needed. An assessment of participants in the CL program had not been done at the study hospital in the past 5 years.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.